Article Text

Abstract
Background and purpose: Hyperdense middle cerebral artery sign (HMCAS) on CT is a well known indication of thromboembolic arterial occlusion. Its disappearance after thrombolytic therapy is poorly described. Taking the rate of HMCAS disappearance as a surrogate for MCA recanalisation, its prognostic value after intravenous thrombolysis was examined.
Methods: 1905 stroke patients with HMCAS on admission CT scan in the Safe Implementation of Treatment in Stroke-International Stroke Thrombolysis Register (SITS-ISTR) were studied. On follow-up CT scans 22–36 h after thrombolysis, HMCAS disappeared in 831 cases, persisted in 788 and was uncertain in 122; follow-up CT was not done in 164 cases.
Results: Patients whose HMCAS disappeared were younger (median age 67 years vs 69 years for persistent; p = 0.03), with milder stroke (admission National Institute of Health Stroke Scale (NIHSS) score was 16 vs 17; p<0.005) and were less likely to have early infarct signs on admission CT (26% vs 33%; p<0.005). Patients with disappearing HMCAS were more likely to have early improvement in NIHSS score (median improvement 2 vs 0 at 2 h; 4 vs 1 at 24 h), be independent at 3 months (42% vs 19%), with fewer deaths (15% vs 30%) than those with persistent HMCAS. In multivariate analysis, HMCAS disappearance independently predicted functional independence and survival. Early NIHSS improvement independently predicted HMCAS disappearance.
Conclusions: HMCAS disappeared after intravenous thrombolysis in about half of cases and these patients had twice as good outcomes compared with those with persistent HMCAS. The prognosis in patients with MCA occlusion that persists after intravenous thrombolysis is poor, which may indicate the need for an alternative treatment approach to this subgroup.
Statistics from Altmetric.com
In acute ischaemic stroke, hyperdense middle cerebral artery sign (HMCAS) on admission CT scan is a known indication of middle cerebral artery occlusion.1–5 Its disappearance after thrombolytic therapy implies vessel recanalisation, as verified by cerebral angiography in observational studies.1 2 6 HMCAS disappearance on follow-up CT scan may be associated with better outcome.7 HMCAS on admission CT is associated with other early infarct signs,8 9 poor prognosis in patients who do not receive thrombolysis10 as well as in patients undergoing intravenous thrombolysis,11–13 and with higher probability of haemorrhagic transformation14 15 after intravenous thrombolysis, while intra-arterial thrombolysis demonstrates more encouraging outcomes in non-randomised studies.16–18 There are limited data on the rate of disappearance of HMCAS after intravenous thrombolysis, and its association with neurological and functional outcome. Information on intravenous thrombolysis in patients with HMCAS would be useful as the effectiveness of intravenous thrombolysis in these patients has been questioned and it is uncertain whether intra-arterial interventions should be a firstline therapy.18 Alternatively, intra-arterial interventions such as thrombectomy could be considered for patients with failed intravenous thrombolysis. The aim of this study was to examine the rate of HMCAS disappearance and its prognostic value after intravenous thrombolysis.
METHODS
The study cohort consisted of 1905 stroke patients with HMCAS on admission CT scan who were registered in the Safe Implementation of Treatment in Stroke-International Stroke Thrombolysis Register (SITS-ISTR) database. SITS-ISTR is an international ongoing internet based open database of stroke thrombolytic treatment. For this study we used the data collected prospectively between December 2002 and October 2006. The structure of the database and the main results from the observational Safe Implementation of Thrombolysis in Stroke- MOntoring STudy (SITS-MOST) were reported previously.19 Ethics approval was provided in each participating country in accordance with national legislation. All patients registered were treated with intravenous alteplase (Actilyse, Boehringer Ingelheim GmbH, Germany). The study protocol was based on standard guidelines for intravenous thrombolysis, with pretreatment CT to exclude haemorrhagic stroke and stroke mimics and initiation of treatment within 3 h of stroke onset. The register contains baseline data, results of follow-up neurological assessment and relevant findings of CT scans, inhospital treatment and 3 month modified Rankin score. Baseline records included chronology (time of stroke onset, admission, imaging, start of treatment), demographic data, patient’s weight, stroke risk factors (hypertension, hyperlipidaemia, smoking, atrial fibrillation, congestive heart failure, history of previous stroke, pre-existing disability); pre-stroke medications (antiplatelet therapy, anticoagulants, antihypertensive treatment); admission blood pressure, plasma glucose and cholesterol levels; and results of neurological assessment and CT scanning. Neurological status was estimated by National Institute of Health Stroke Scale on admission and at 2 h, 24 h and on day 7.
Clinical subtypes of stroke were not available directly from the database. Nevertheless, in order to examine the rate of total anterior circulation infarct (TACI) syndrome, which is a clinical presentation of proximal MCA occlusion, it was derived as an approximation from the baseline National Institute of Health Stroke Scale (NIHSS) records. The syndrome was defined as a combination of higher cerebral dysfunction, homonymous visual field defect, and ipsilateral motor and/or sensory deficit of at least two areas of the face, arm and leg.20 Presence of TACI syndrome was set with the assumption that facial palsy and sensory deficit were ipsilateral to the motor deficit in the arm and leg.
Stroke aetiology was established in accordance with the TOAST classification. Admission CT scans were evaluated for the presence of HMCAS and ischaemic signs. Follow-up CT scans were performed within 22–36 h of stroke (or earlier if clinically indicated) and evaluated for the presence of HMCAS, ischaemic signs, infarct swelling and intracerebral haemorrhage. Outcomes were independence (modified Rankin Score (mRS) 0–2 on day 90) and death (mRS = 6 on day 90). Unfavourable outcome was defined as death or dependency (mRS 3–6). Symptomatic intracerebral haemorrhage (SICH) was defined as local or remote type 2 parenchymal haemorrhage on the 22–36 h post-treatment imaging scan, accompanied by deterioration of baseline NIHSS score ⩾4 points or death within 24 h after thrombolysis (SITS-MOST definition).19 Additionally, we used a definition from previous randomised controlled trials: any haemorrhage on follow-up imaging combined with at least 1 point deterioration on NIHSS or death until day 7. Neurological improvement was estimated by the difference between admission and follow-up NIHSS scores. Relation of extent of neurological improvement to outcome was estimated in the whole HMCAS group at several levels of NIHSS score difference. Dramatic neurological improvement was defined as NIHSS score 0, 1 or improvement ⩾821 from baseline score at a follow-up time point.
HMCAS disappearance (HMCAS-D) and persistence (HMCAS-P) were identified on follow-up CT scans.
Statistical analysis
Baseline data, admission clinical variables, stroke aetiology, results of neurological assessment, other CT findings and outcomes were compared between the HMCAS persistence and disappearance groups. Multivariate analyses were performed to identify prognostically important factors for HMCAS disappearance and to identify prognostic significance of HMCAS disappearance on main outcomes. Prognostic significance of HMCAS disappearance was adjusted for stroke risk factors and aetiology, onset to treatment time, admission NIHSS score, blood glucose and extent of immediate NIHSS improvement at 2 h. Statistical analysis was performed with Statistica 6.0 software. Estimation of percentages was based on reported cases only, excluding missing data. For univariate comparison between HMCAS-D and HMCAS-P subgroups, we used the t test for numerical data, the Mann–Whitney test for scores and non-parametrically distributed numerical variables, and the χ2 test (with Yates correction for 2×2 tables or, in case of small expected frequencies, Fisher’s exact test) for proportions. For multivariate analysis, we performed multiple logistic regression to define independent predictors of functional outcome. Taking into account multiple comparisons, significance level for univariate testing was accepted as p<0.01.
RESULTS
Of 1905 patients with HMCAS on admission CT scans, the sign disappeared in 831 (48%), persisted in 788 (45%) and was uncertain in 122 (7%) on 22–36 h follow-up CT scans. In the remaining 164 cases, follow-up CT was omitted. The subgroup with uncertain HMCAS on follow-up CT scan demonstrated a trend to lower independence rate at 3 months (24.6% vs 31.2%; p = 0.1) and the same death rate (23.4% vs 23.6%; p = 0.9) than the rest of the population of patients with HMCAS on admission CT scan (n = 1783). The subgroup with missing follow-up CT scans had a higher independence rate (40.6% vs 29.8%; p = 0.01) and non-significantly more deaths (28% vs 23%, p = 0.2) than the rest of the population of patients with HMCAS on admission CT scan (n = 1741). We decided to exclude the missing and uncertain groups from further analyses, given the similarity of outcomes between these groups and the rest of the group of patients with admission HMCAS.
Results of univariate comparison of HMCAS-D and HMCAS-P subgroups are shown in tables 1 and 2. Virtually no difference was found regarding past medical history and chronology. In particular, the onset to imaging and treatment times were the same in both groups. Patients with HMCAS-D had a slightly lower median age, slightly lower admission NIHSS score and fewer ischaemic signs on admission CT. The proportions of patients with a TACI syndrome were approximately equal in subgroups with persistent and disappeared HMCAS on follow-up CT (no statistically significant difference, table 2).
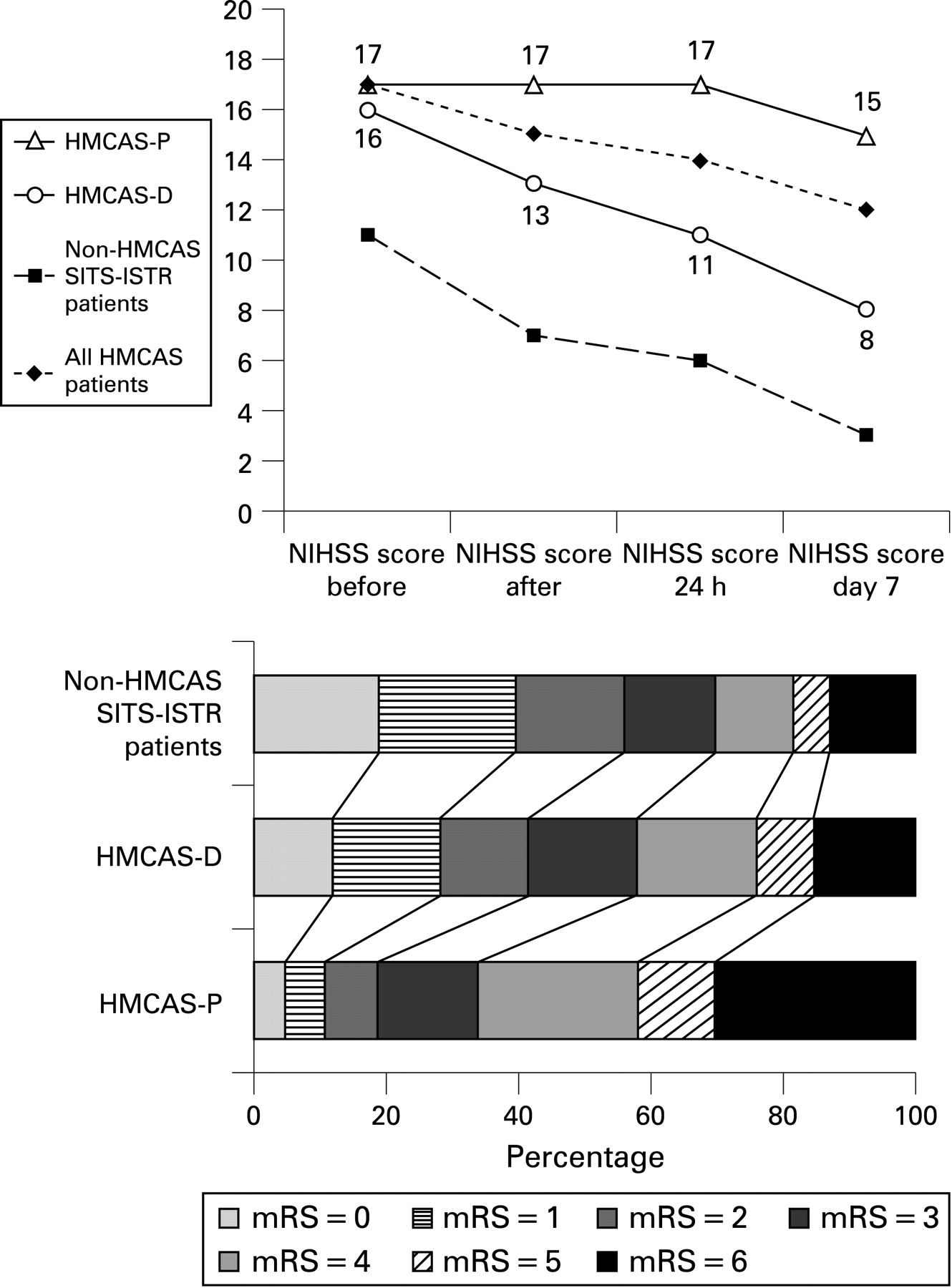
The HMCAS-D subgroup had borderline three times higher rate of SICH according to the SITS-MOST definition compared with the HMCAS-P subgroup, but a lower rate of SICH according to the randomised controlled trials definition. Despite a higher rate of type 2 parenchymal haemorrhage, the HMCAS-D subgroup demonstrated a much more favourable NIHSS profile (fig 1). Twice as many achieved functional independence at 3 months with half as many deaths as in the HMCAS-P subgroup. Outcomes were approaching those for patients without HMCAS on the baseline scan (fig 1). Outcomes of non-HMCAS patients in the SITS register have been published elsewhere.22 Early neurological improvement by ⩾4 points NIHSS at 2 h (post-treatment) was twice as common, and dramatic neurological improvement at 2 h occurred three times more often in HMCAS-D patients. Median change of NIHSS score from baseline in HMCAS-D and HMCAS-P patients was 2 versus 0 at 2 h and 4 versus 1 at 24 h (p<0.001).

In our multivariate analysis, stroke risk factors, TOAST subgroups or admission blood glucose did not appear to predict good outcome. HMCAS disappearance was one of the strongest predictors of good functional outcome at 3 months (odds ratio 2.26, 95% confidence interval 1.68 to 3.05; p<0.001); other independent predictors of outcome in HMCAS patients were age, admission NIHSS score and extent of neurological improvement at 2 h. Admission NIHSS score and extent of neurological improvement at 2 h independently predicted HMCAS disappearance.
Based on the association between 2 h NIHSS improvement and 3 month outcome in patients with HMCAS disappearance, we categorised the 2 h NIHSS difference to identify a suitable cut-off level to be used clinically for prediction of outcomes (table 3, fig 2). The proportion of patients with favourable outcomes increased sequentially with each point NIHSS improvement at 2 h. However, the most favourable outcomes were observed in those who demonstrated dramatic neurological improvement at 2 h: 75.2% (n = 94) were independent and 4.8% (n = 6) had died after 3 months compared with 25.7% (307) and 24.4% (292), respectively, of those without dramatic improvement (p<0.001).

{kind=link}
{kind=link}
Repeated multivariate analyses were performed, including 2 h NIHSS improvement strata (decline in NIHSS score ⩾4, ⩾3, ⩾2 or ⩾1 from baseline) together with previously determined prognostically important factors (baseline NIHSS score, age and HMCAS disappearance). On testing various cut-off levels, we found that any improvement in NIHSS score from baseline (ie, difference between baseline and 2 h NIHSS scores of at least 1) was associated with good functional outcome.
DISCUSSION
To our knowledge, this is the largest study examining the rate of HMCAS disappearance and its prognostic value in patients treated with intravenous thrombolysis. HMCAS is a well known sign of MCA occlusion and a valuable, reliable and quick to assess prognostic sign in its own right. Its clinical use may become more limited following the development of multimodal imaging but its value when present should not be underestimated. However, inability to demonstrate details of occlusion, such as tandem or T-shaped clot, in occasional circumstances where this detail might be helpful, is the main weakness of plain CT in the setting of MCA stroke.
We observed that the HMCAS disappeared after intravenous thrombolysis on follow-up CT scan at 22–36 h after stroke onset in about half of patients. These patients showed more rapid neurological improvement and had better functional outcome, as measured by mRS 0–2, and lower mortality at 3 months compared with patients in whom the HMCAS persisted. In the multivariate analysis of outcome predictors, disappearance of the HMCAS appeared to be one of the independent predictors of 3 month independence and reduced mortality. These results suggest that HMCAS-D patients are adequately recanalised as their outcomes were comparable with patients without the HMCAS on admission CT after adjustment for their initial stroke severity (fig 1). In contrast, HMCAS-P patients had very poor short and long term outcomes after intravenous thrombolysis. However, HMCAS disappearance after 22–36 h serves only as a landmark of large artery recanalisation and may be demonstrated too late to be a criterion for clinical decisions.
Some of the baseline parameters differed between the HMCAS-D and HMCAS-P subgroups but these differences cannot be used in clinical practice as prognostic markers for persistence because they were marginal. Patients with persistence were 2 years older, had 1 point more median baseline NIHSS and more often had signs of current infarction than those with disappearance, which may indicate that HMCAS-P patients had less favourable baseline data despite being imaged and treated at the same time after stroke. We hypothesised that the disappearance of HMCAS on follow-up CT scans indicated vessel recanalisation. The clinical course and outcome of the HMCAS-D subgroup support our hypothesis. When we followed the clinical course of all HMCAS patients, we considered whether absence of neurological improvement at 2 h might help to identify those in whom the HMCAS was likely to persist. We observed that HMCAS persisted in more than half of patients with any NIHSS improvement at 2 h (table 3). In the multivariate analysis, 2 h NIHSS changes, by as little as 1 point, appeared as one of the significant predictors for HMCAS disappearance but the overlap was substantial. In this setting, lack of neurological improvement cannot be the basis for the decision about additional intervention as this approach fails to identify almost half of patients with a poor prognosis in the HMCAS-P subgroup. Hence it seems reasonable to take patients with identified MCA occlusion and no clinical improvement after intravenous thrombolysis directly to the angiosuite in order to perform DSA and attempt mechanical recanalisation. This approach may be suggested for testing in a randomised controlled trial.
SICH, according to the SITS-MOST definition, was comparatively uncommon in the HMCAS-P subgroup while that of the HMCAS-D subgroup was close to the SICH rate observed in the SITS-MOST study.19 This finding may support the previously discussed hypothesis that recanalisation of an occluded vessel predisposes to subsequent haemorrhage.15 23–25 The overall rate of severe ICH among HMCAS-D patients, which fall into SICH by the SITS-MOST category, was still small, hence it did not influence the generally favourable clinical course and proportion of good outcome in this subgroup. As for the higher prevalence of SICH by the randomised controlled trials definition in HMCAS-P patients, this observation may be partly explained by a large volume of necrotic infarction in patients with persistent MCA occlusion, which results in minor intracerebral haemorrhage.
Our results cannot provide an explanation for the initial small difference in baseline NIHSS scores between the HMCAS-D and HMCAS-P subgroups, suggesting that some other unrecorded factors may play a role, one of which could be, for instance, composition of the clot.26 We only recorded the presence of HMCAS, not its site or extent (it is possible that HMCAS-P patients had longer clots, or more proximal clots, that involved the ICA/proximal MCA, whereas HMCAS-D patients only had insular branch MCA clots, hence accounting for the difference in visible infarction and features suggesting more severe strokes in HMCAS–P patients). However, the observation that the difference in TACI syndromes between HMCAS-D and HMCAS-P subgroups was small and statistically insignificant speaks against this being a major explanation for the differences in outcome. The trend for more patients with large vessel disease in the HMCAS-P subgroup is in line with poorer outcomes after intravenous thrombolysis when MCA occlusion is combined with ICA obstruction.27 Moreover, one could speculate that these patients have a higher incidence of underlying arterial stenosis and subsequent re-occlusion after successful thrombolysis.
There are some limitations to our study. Firstly, this is an observational unblinded study. Secondly, approximately 12% of follow-up scans were missing. Thirdly, we did not have CT or MR angiography or transcranial Doppler data for most of these patients (only 11% had CTA or MR angiography) to examine whether the disappearance of the sign correlated with vessel recanalisation, although that was not the aim of our study. Fourthly, follow-up CT scans were performed between 22 and 36 h after recombinant plasminogen activator treatment, as standard protocol. Therefore, we do not know how quickly the HMCAS disappeared, only what proportion had disappeared by 22–36 h. The scans were read by local doctors with wide variation in experience and expertise for early stroke CT assessment, so some unintentional errors could have occurred. It is possible that the NIHSS scores were influenced by knowledge of CT findings since the physicians were unblinded to the CT scans. Despite these limitations, this is the largest study on early follow-up of HMCAS patients given intravenous thrombolysis. Previous studies did not have more than a few hundred patients,2 12 13 and in some cases less than a hundred patients were analysed,1 11 24 although in these studies the scans were read centrally, usually by one expert, resulting in less potential noise in the HMCAS assessment.
CONCLUSIONS
The admission hyperdense MCA sign disappears on 22–36 h CT scans after intravenous thrombolysis in almost half of all cases. The proportion of functionally independent patients in the HMCAS disappearance subgroup was more than double and mortality was less than half compared with the HMCAS persistence subgroup. A higher prevalence of type 2 parenchymal haemorrhage in the HMCAS disappearance subgroup did not influence overall favourable 3 month outcome. The prognosis in patients with MCA occlusion that persists after intravenous thrombolysis is poor, which may indicate the appeal for alternative treatment approaches in this subgroup.
Acknowledgments
Scientific Committee of SITS International: Nils Wahlgren (chair), Antoni Davalos, Gary A Ford, Martin Grond, Werner Hacke, Michael Hennerici, Markku Kaste, Vincent Larrue, Kennedy R Lees, Risto Roine and Danilo Toni.
REFERENCES
Footnotes
Competing interests: NA is an employee of SITS International. SITS International receives an unrestricted grant from Boehringer-Ingelheim. RvK has received honoraria for lectures and/or for advisory boards from Boehringer-Ingelheim, Sanofi-Aventis, Astra-Zeneca, Bayer, Pfizer, NovoNordisk, Astellas, Terumo, Paion and Novartis. JMW works for the University of Edinburgh and provided imaging expertise for the SITS-MOST registry, including design of the image data acquisition and reading of scans submitted to SITS-MOST for expert review. She has received honoraria only for providing expert scan interpretation for SITS-MOST from SITS International who are supported by Boehringer-Ingelheim. LT has received honoraria for lectures and financial support for research nurses from Boehringer-Ingelheim. NW is chairman of SITS International. SITS International receives an unrestricted grant from Boehringer-Ingelheim. NW has received honoraria for lectures and/or for advisory boards from Boehringer-Ingelheim, Sanofi-Aventis, Astra-Zeneca, Bayer and Thrombogenics.
Funding: SITS-ISTR is funded by an unrestricted grant from Boehringer-Ingelheim (BI), and by a grant from the European Union Public Health Authority (PHEA). Preparation of this paper was independent of the funding organisation. The views expressed are those of the authors. Uppsala Clinical Research (UCR), Sweden, develops, maintains and upgrades the software for SITS register in close collaboration with SITS.
Ethics approval: Ethics approval was provided in each participating country in accordance with national legislation.
See Editorial Commentary, p 248