Article Text

Abstract
Objective To investigate whether or not the lesions in sporadic amyotrophic lateral sclerosis (ALS) originate from a single focal onset site and spread contiguously by prion-like cell-to-cell propagation in the rostrocaudal direction along the spinal cord, as has been hypothesised (the ‘single seed and simple propagation’ hypothesis).
Methods Subjects included 36 patients with sporadic ALS and initial symptoms in the bulbar, respiratory or upper limb regions. Abnormal spontaneous activities in needle electromyography (nEMG)—that is, fibrillation potentials, positive sharp waves (Fib/PSWs) or fasciculation potentials (FPs)—were compared among the unilateral muscles innervated by different spinal segments, especially between the T10 and L5 paraspinal muscles, and between the vastus medialis and biceps femoris. Axon length and the proportion of muscle fibre types, which are both related to motoneuronal vulnerability in ALS, are similar in the paired muscles.
Results Fourteen of 36 patients showed a non-contiguous distribution of nEMG abnormalities from the onset site, with skipping of intermediate segments. In eight of them, the non-contiguous pattern was evident between paired muscles with the same motoneuronal vulnerability. The non-contiguously affected lumbosacral lesions involved motoneuron columns horizontally or radially proximate to one another, appearing to form a cluster in four of the eight patients. FPs, known to precede Fib/PSWs, were shown more frequently than Fib/PSWs in all the lumbosacral segments but L5, suggesting that 2nd hits occur at L5 and then spread to other lumbosacral segments.
Conclusions In sporadic ALS, the distribution of lower motoneuron involvement cannot be explained by the ‘single seed and simple propagation’ hypothesis alone. We propose a ‘multifocal hits and local propagation’ hypothesis instead.
- Motor Neuron Disease
- ALS
- EMG
- Neurophysiology
- Clinical Neurology
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is an incurable progressive neurodegenerative disease in which both the upper (UMN) and lower motoneurons (LMN) are diffusely involved at the end. Recent biological studies have demonstrated the remarkable concept of ‘prion-like propagation’ of pathogenic proteins, such as tau or α-synuclein, in neurodegenerative diseases.1 ,2 According to this hypothesis, the pathogenic proteins are transferred from diseased cells to neighbouring healthy cells; this intercellular transfer then leads to spreading of the lesion. In ALS, in vitro studies have indicated that newly formed aggregates of SOD1, TDP-43 or toxic RNA conformation can act as templates for the subsequent misfolding of the respective native proteins,3–5 and that aggregated SOD1 can be intercellularly transferred in cultured cells.6 These suggest that the mechanism of prion-like cell-to-cell propagation also underlies the progression of ALS.
The clinical symptoms of most ALS patients start focally, which had already been confirmed both electrophysiologically7 and pathologically.8 ,9 As we have reviewed in the previous article,10 recent clinical observations have demonstrated that the clinical symptoms spread contiguously from the onsets into the following broadly divided body regions: the bulbar region, upper limbs, trunk and lower limbs.11–14 This has prompted us to suppose that ALS lesions simply propagate from a single ‘seed’ to adjacent cells in a domino-like manner (ie, the ‘single seed and simple propagation’ hypothesis). Alternatively, it can rest on anatomical proximity with the spreading of ALS lesion from the onset site by diffusion of soluble toxic factors in the extracellular matrix.15 On the other hand, up to about 30% of sporadic ALS patients have also been found to show non-contiguous spread of symptoms from the bulbar region to the lower limbs or vice versa, skipping the upper limbs and trunk.14 ,16 However, compensatory re-innervation by the remaining motoneurons can mask the manifestation of clinical signs until more than one-third of the LMNs for a given muscle are lost.17 Therefore, whether the lesions actually spread non-contiguously among the spinal segments remains unclear.
Needle electromyography (nEMG) can sensitively detect LMN involvement from each segment separately, even in the presymptomatic stage. For this reason, it is a powerful method for investigating whether or not ALS lesions spread contiguously along the spinal segments. In this study, we used nEMG in the early stage of ALS to demonstrate that LMN involvement cannot be necessarily explained by the ‘single seed and simple propagation’ hypothesis. We then propose a hypothesis of ‘multifocal hits and local propagation.’
Subjects and methods
Subjects
We designed this study to investigate whether LMN involvement in sporadic ALS spreads contiguously in the rostrocaudal direction from the onset site. Therefore, of 66 consecutive patients with suspected ALS referred to our hospitals from March 2011 to April 2012, 14 patients with lower limb onset were excluded. One patient with a family history of ALS was also excluded. Forty-two of the remaining 51 patients met the revised El Escorial criteria18 for clinically definite, clinically probable or clinically probable laboratory-supported ALS, although two patients were excluded because their MRIs indicated lumbar spinal disease, which can influence the results of nEMG. Thus, 40 sporadic ALS patients with bulbar, upper limb, or respiratory symptoms at onset were ultimately included in this study. None of these 40 patients had diabetes or any other complicating neuropathies, which were confirmed by nerve conduction studies (performed on their unilateral median, ulnar, tibial, peroneal and sural nerves).
Selection of muscles to be examined
Motoneurons with longer axons,19 ,20 larger motoneurons9 and fast-fatigable motoneurons21 have been described as more vulnerable to damage from ALS. If the pathological process begins at the same time in individual motoneurons with different degrees of vulnerability, then motoneurons that are more vulnerable will degenerate faster than those that are more resistant. Thus the pattern of nEMG abnormalities should be influenced by differences in motoneuronal vulnerability. Therefore, to establish adequate milestones for lesion spreading, we selected two pairs of muscles innervated from different spinal segments but with similar degrees of motoneuronal vulnerability; that is, the length of the innervating motor axons and the ratio of type I muscle fibres differ little between the paired muscles (see online supplementary figure S1). One pair—T10 paraspinalis (T10PS; type I fibre ratio: 62.0% in men, 67.8% in women) and L5 paraspinalis (L5PS; 63.6–65.0%)—was selected from the trunk.22 The other pair—the deep layer of the vastus medialis (VM) (innervating segment: L3/4; type I fibre ratio: 61.5%) and the long head of the biceps femoris (BF; L5/S1, mainly S1; 66.9%)—was selected from the thigh.23–27
If a focal ALS lesion spreads contiguously in the rostrocaudal direction along the spinal segments, nEMG abnormalities in the paired muscles should be found in the muscle innervated by the rostral segment earlier than in the muscle innervated by the caudal segment (the ‘contiguous pattern’ in online supplementary figure S1). On the other hand, if the abnormalities are observed only in the muscle innervated by the caudal segment while the muscle of the rostral segment remains intact (the ‘non-contiguous (skipping) pattern’ in online supplementary figure S1), the results cannot be attributed to differences in motoneuronal vulnerability. We also examined the first dorsal interosseous (FDI; mainly innervating segment: C8), L3 paraspinalis (L3PS), rectus femoris (RF; L3/4), tibialis anterior (TA; L4/5, mainly L5) and medial head of the gastrocnemius (GC; S1/2, mainly S1).23–26
Needle electromyography
Spontaneous EMG activities were detected with a conventional concentric needle electrode (recording surface area: 0.3 mm2) in the above-mentioned muscles on the ipsilateral side of symptom onset in the upper limb onset patients and on the right side in the patients with bulbar or respiratory onset. For evaluation of paraspinal muscles, we examined the multifidus muscles, which are innervated by a single segment.28
Fibrillation potentials and positive sharp waves (Fib/PSWs) were explored at 10 different sites in each muscle. Fib/PSWs were diagnosed to be pathological only when they were identified at more than two different sites within the muscle. The fasciculation potential (FP) was defined as a potential that was similar in shape to the motor unit potential (MUP) and fired in a highly irregular pattern, often with a clustering of discharges. We identified FPs only when potentials of the same shape appeared at least twice. To detect FPs, we observed spontaneous activity at one site in each muscle for 60–90 s, which is sufficiently long enough to confirm the reproducibility of FPs.29 Any persistence of voluntary MUPs was considered to render the identification of FPs impossible. We considered the examined muscles to be involved if Fib/PSWs, FPs or both were observed. Considering their higher objectivity beyond multicentre and burdens of patients, only spontaneous activities were adopted to prove LMN involvements in this study.
All EMG examinations were performed by proficient electromyographers with at least 5 years of professional EMG experience (TS, TK, KS and YN).
Data analysis
Frequencies of the presence of abnormal spontaneous EMG activity were compared among the examined muscles by performing multiple comparisons with Fisher's exact probability test and the p value adjustment method of Holm. p Values less than 0.05 were considered to be significant.
Standard protocol approvals, registrations and patient consents
The local ethics committees of Tokyo Medical and Dental University School of Medicine, Chiba University Graduate School of Medicine, Kyoto Prefectural University of Medicine, Musashino Red Cross Hospital, Kanto Central Hospital and Nakano General Hospital approved this study. All patients gave us informed consents for the procedures.
Results
Of the 40 patients with sporadic ALS included in this study, we ultimately analysed data from 36 patients (23 men, 13 women) because sufficient data for the paired paraspinal and thigh muscles were not obtained in 4 patients. The ages of 36 patients ranged from 41 years to 79 years (mean 63.3). The diagnoses were definite ALS in 8 patients, probable in 14 and probable-laboratory-supported in 14 according to the revised El Escorial criteria. Symptom onset occurred in the bulbar region in 10 patients, in the upper limb in 25 patients and as respiratory symptoms in 1 patient. The mean duration from symptom onset to the nEMG study was 16.9 months (range 3–84).
The full nEMG data for the 36 patients are shown in figure 1, online supplementary figure S2A,B. Abnormal spontaneous EMG activity was present in the FDI of all 36 patients. The distribution patterns of nEMG abnormalities among the spinal segments could be divided into three types: diffuse, contiguous and non-contiguous (skipping) patterns. The diffuse pattern was observed in 19 patients (53%); of these, 13 (patients 1–13) showed abnormal nEMG findings at all examined muscles and 6 (patients 14–19) showed abnormalities at every examined spinal segment, although not at all muscles. The contiguous pattern was found in three patients (8.3%; patients 20–22) in whom abnormal findings were detected in all examined segments except S1—the most remote segment from the onset site. One of these three patients (patient 22) also showed the contiguous pattern in the thigh muscle pair; that is, an abnormality was evident in VM but not in BF. The non-contiguous (skipping) pattern was found in 14 patients (39%; patients 23–36), in whom abnormal spontaneous activities were detected from C8 to more caudal segments with skipping of intermediate segments such as T10 or L3/4. Representative nEMG findings of the non-contiguous pattern in a patient with bulbar onset (patient 27) are shown in figure 2.

Distribution patterns of needle electromyography (nEMG) abnormality in all patients. Closed squares: abnormal spontaneous EMG activity present. Open squares: abnormal spontaneous EMG activity absent. Squares with oblique line: data not available. (A) Diffuse pattern. (B) Contiguous pattern. (C) Non-contiguous (skipping) pattern. Note that the rostrally absent and caudally present spontaneous activity pattern between paired muscles with the same motoneuronal vulnerability is evident in the paraspinal muscle pair (green, patients 23–27) and the thigh muscle pair (red, patients 27–30) in 8 of 14 patients with the skipping pattern. The non-contiguous (skipping) pattern was present in both muscle pairs in patient 27.

Representative needle electromyography (nEMG) finding in the patient with non-contiguous pattern. nEMG finding of patient 27 whose onset was bulbar symptoms. Positive sharp waves (first dorsal interosseous (FDI), L5PS and tibialis anterior (TA)) or a fasciculation potential (biceps femoris (BF)) are present with skipping of the muscles innervated by intermediate segments. Note that the non-contiguous (skipping) distribution pattern is evident between the muscles of the paraspinal (T10PS and L5PS) and thigh (vastus medialis (VM) and BF) pairs. Red type indicates nEMG abnormalities.
Eight of the 14 patients also exhibited the non-contiguous pattern in the paired muscles; of these, five (patients 23–27) showed the pattern in the paraspinal muscle pair (involvement of L5PS with skipping of T10PS) (table 1A), four (patients 27–30) showed the pattern in the thigh muscle pair (involvement of BF innervated by S1 with skipping of VM innervated by L3/4) (table 1B). One of the eight patients (patient 27) showed this pattern in both pairs.
Frequencies of nEMG abnormality patterns in paired muscles among 14 patients with a non-contiguous (skipping) pattern
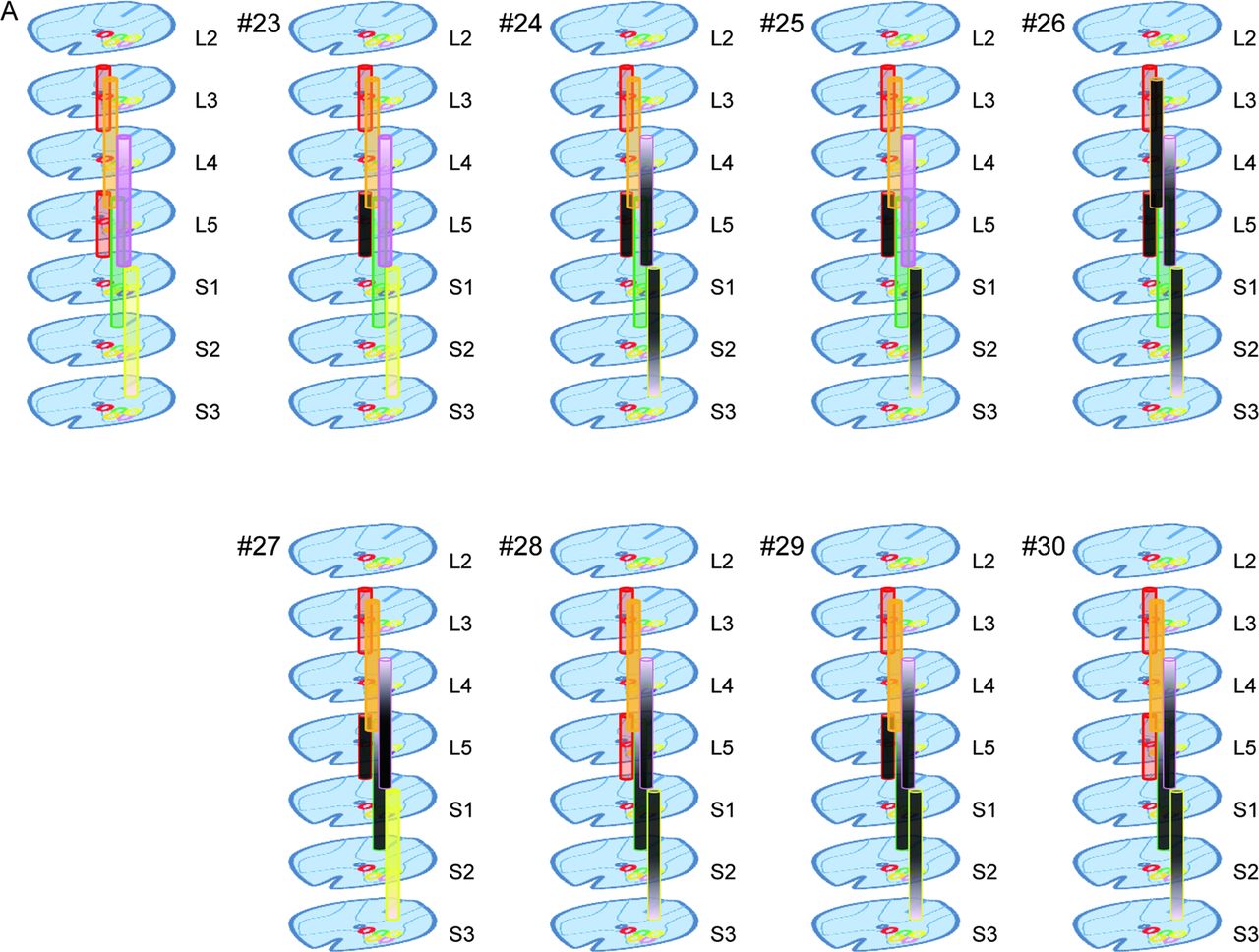
In order to consider whether there is a local propagation of the non-contiguously affected lumbosacral lesion, we used schematics to examine the anatomical distributions of the involved motoneuron pools of the lumbosacral muscles in the eight patients who exhibited the skipping pattern in the paired muscles (figure 3).23–26 ,30 ,31 The involved motoneuron pools were located in close horizontal or radial proximity to one another in five patients (patients 26–30) and appeared to form a cluster in four patients (patients 27–30). By contrast, the involved motoneuron pools were not horizontally contiguous in two patients (patients 24–25). The one remaining patient (patient 23) had only one lesion in the lumbosacral muscles.

Schematic diagrams of motoneuron pools of the examined muscles in the lumbosacral cord (A) and their patterns of involvement in eight patients showing the non-contiguous (skipping) pattern in the paired muscles (patients 23–30). The locations of motoneuron pools innervating each muscle were taken from refs 23–26 ,30 and 31. Note that the involved motoneuron pools (darkly shaded) appear to neighbour one another in 3-dimensional anatomy, and appear to form a cluster for four patients (patients 27–30) in particular. VM (orange column), vastus medialis deep layer; RF (orange column), rectus femoris; L3 PS (upper red column), paraspinal muscle at L3 level; TA (pink column), tibialis anterior; L5 PS (lower red column), paraspinal muscle at L5 level; BF (green column), biceps femoris long head; GC (yellow column), gastrocnemius medial head.
Excluding FDI, which was involved in all patients, the percentage of patients with nEMG abnormalities was the highest in TA (13/17, 76.5%) and L5PS (11/17, 64.7%) and was the lowest in RF and VM (2/17, 11.8%) (figure 4). Pairwise comparisons among the muscles showed statistically significant differences in proportions between the muscles innervated by L3/4 and L5: RF and TA (p=0.01), RF and L5PS (p=0.03), VM and TA (p=0.01), and VM and L5PS (p=0.03). There were no statistically significant differences in other pairs of muscles except those including FDI.
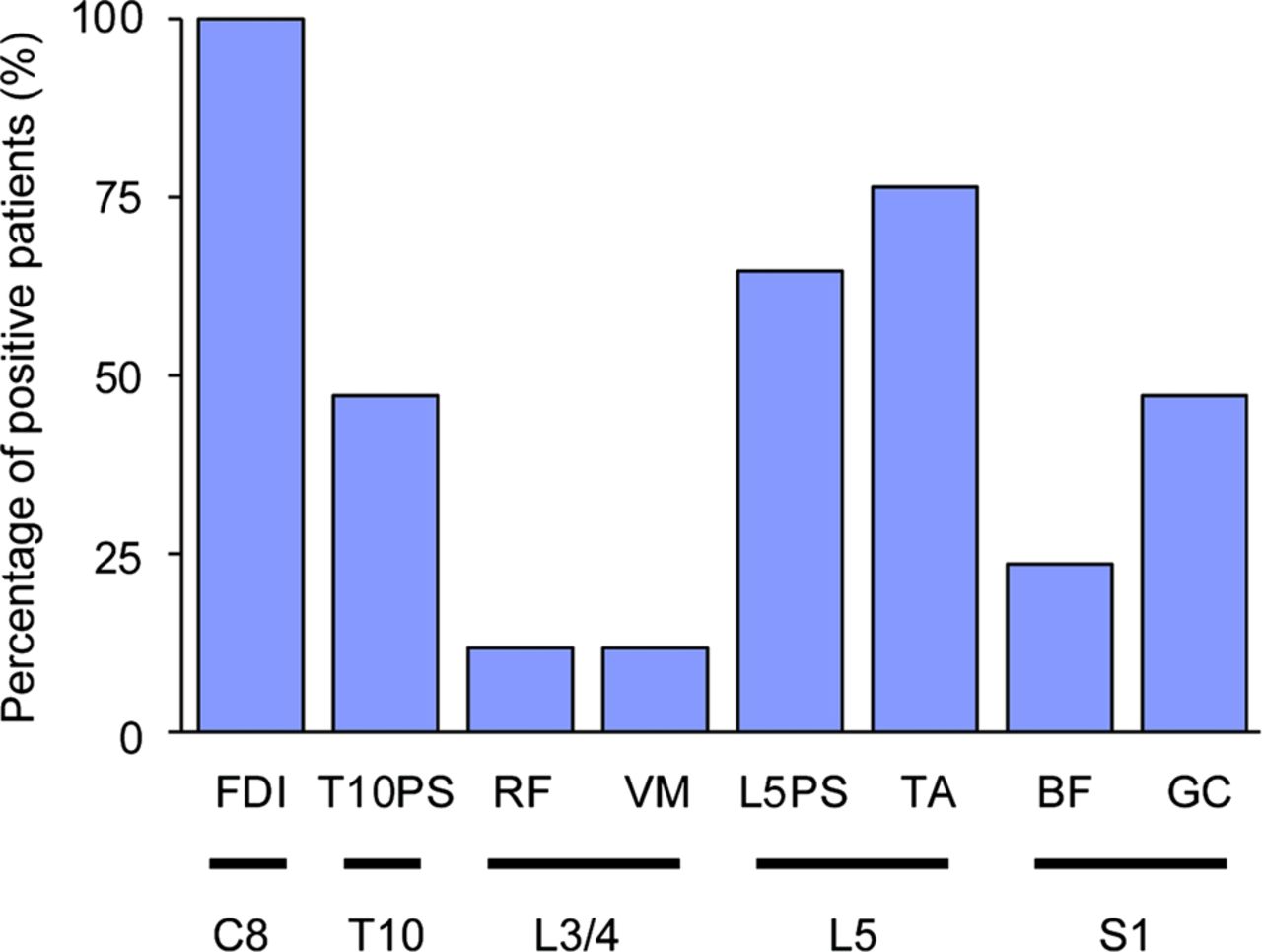
Frequency of needle electromyography abnormality of each muscle in the patients with contiguous and non-contiguous distribution patterns. With the exception of first dorsal interosseous (FDI) which, as the most rostral muscle, was affected in all patients, the highest frequencies were found in the muscles innervated by L5 and the lowest in the muscles innervated by L3/4. The differences were statistically significant (p<0.05, Fisher's exact probability test using the p value adjustment method of Holm). Note that the frequencies are almost same between L5PS and tibialis anterior (TA).
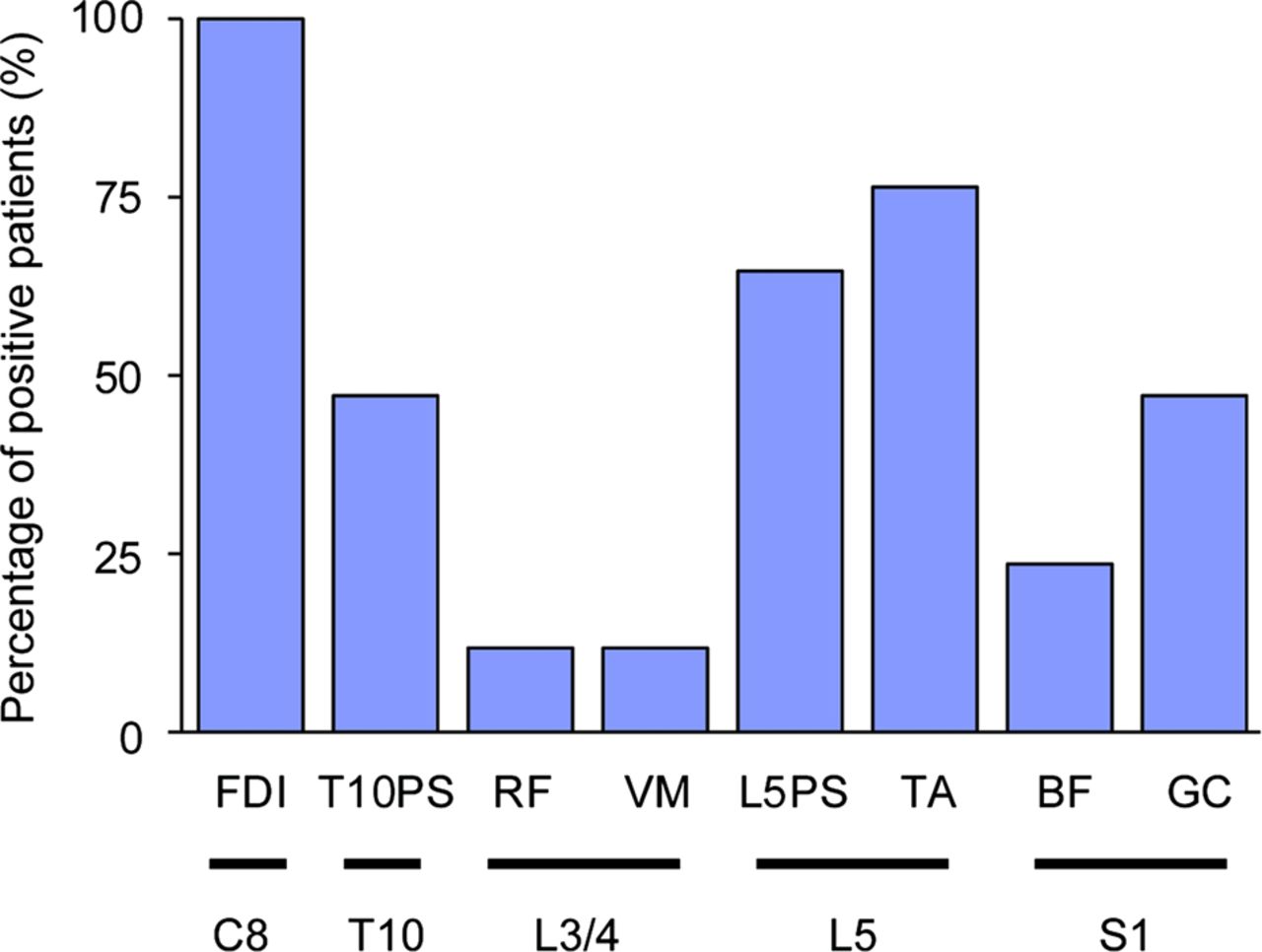
We also investigated and compared the frequency of Fib/PSWs and that of FPs in every muscle of all included patients (figure 5). Fib/PSWs were more frequently observed than FPs in FDI (C8), which was the onset region in most of the included patients. To the contrary, FPs were dominantly observed than Fib/PSWs in RF or VM (L3/4) and BF or GC (S1), away from the onset region. However, TA and L5PS, both of which are innervated by L5, showed Fib/PSWs less rarely than FPs.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The comparison of frequencies between fibrillation potentials, positive sharp waves (Fib/PSWs) and fasciculation potentials (FPs) of each muscle in all patients. Blue bar: Fib/PSWs, Red bar: FPs. FPs, known to precede Fib/PSWs, were shown more frequently than Fib/PSWs in the all lumbosacral segments but L5, suggesting that L5 segment was involved earlier than other lumbosacral segments.
Discussion
We investigated whether the involvement of LMNs in sporadic ALS spreads contiguously in the rostrocaudal direction from the onset site. If prion-like propagation underlies the progression of ALS and the disease pathology in the first focal lesion propagates to adjacent cells in a cell-to-cell domino-like manner (the ‘single seed and simple propagation’ hypothesis) (see online supplementary figure S3A), involved LMNs should be distributed contiguously from the onset site.
Our nEMG study revealed that more than 50% of patients showed diffuse patterns. They showed weakness or muscle atrophy in lumbosacral regions more frequently than the rest (79% vs 29%). Therefore, they seemed to be in later stages of the disease.
In 14 of 17 patients, after excluding patients with the diffuse pattern, the abnormalities were distributed non-contiguously from the onset site, with skipping of intermediate spinal segments. The non-contiguous distribution of nEMG abnormalities may merely represent false-negative nEMG results in the ‘skipped’ segments where LMNs have in fact been involved. Two kinds of false negatives are conceivable: that based on methodological limitations, and that due to the time lag from molecular disease onset. First, given that a needle electrode has a limited pick-up area, evaluating all motor units (MU) in a muscle is practically impossible. Second, a time lag must exist because many molecular changes occur before they reach a threshold at which spontaneous EMG activities can be detected. Individual LMNs have different vulnerabilities in ALS;9 ,19–21 more vulnerable LMNs will degenerate faster than more resistant ones even if the pathological molecular process begins simultaneously. Therefore, the failure to detect abnormal EMG activities in skipped spinal segments may simply have been caused by the lower vulnerability of neurons at these sites, if less vulnerable LMNs are radially sandwiched by the highly vulnerable LMNs of more rostral and caudal segments.
However, we consider it unlikely that they alone could produce the non-contiguous pattern. The sensitivities for detecting spontaneous EMG activity should be very similar in the two thigh muscles (VM and BF) and in the paraspinal muscles (T10 and L5) we examined. First, this is because the total number of insertions was fixed in every muscle by the same examiner. Second, the motoneuronal vulnerabilities as well as the sensitivities are expected to be nearly identical between the paired muscles because the lengths of their innervating motor axons are very similar and they have similar proportions of type I/II muscle fibres. Taken together, the probability of false negatives should be nearly same between the paired muscles. Therefore, the segmental distribution of ALS lesions can be non-contiguous along the spinal cord in the early stage of the disease (see online supplementary figure S3B).
Krarup claimed that abnormal spontaneous activities in nEMG are not as sensitive as changes in MUPs.32 We have searched these chronic neurogenic changes in VM/RF of the four patients who showed non-contiguous pattern in thigh pair of muscles. Although one patient (patient 28) showed polyphasic MUPs in RF, the other three patients are still classified as non-contiguous pattern with evaluating chronic changes, and therefore, our conclusion remains unchanged. In fact, which kind of neurogenic changes appears the earliest in nEMG of ALS patients still remains controversial. Recently, de Carvalho et al33 have reported that FPs are the earliest changes in ALS patients.
Both the spreading mechanisms of toxic factors, namely, simple diffusion of soluble toxic factors and cell-to-cell propagation from the only onset site are inconsistent with these non-contiguous distributions. The former mechanism should show abnormalities in anatomically proximal segments to onsets such as T10/L3 earlier than L5/S1. Assuming the latter mechanism, it is important to note that the lateral motor columns of the anterior horn innervating distal limb muscles are not structurally contiguous between the cervical and lumbosacral spinal cords.30 By contrast, the medial motor column, which innervates axial muscles, extends contiguously from the lower medulla to the lumbar spinal cord. This indicates that regional spread from FDI to TA needs to have three steps; (1) disease transfer from lateral to medial motor column in cervical segment, (2) caudal propagation along the medial column and (3) disease transfer from medial to lateral motor column in lumbosacral segments. If ALS lesions spread along the medial column in the rostrocaudal direction by cell-to-cell propagation, our results showing the skipping of T10PS or L3PS in 11 of the 14 patients with non-contiguous pattern cannot be explained. Taken together, whatever mechanisms can underlie the consequent spread, we conclude that ALS progression is not explained by single onset site, but by multiple onset sites. This speculation is consistent with the fact that there are ALS patients who have onsets in two regions simultaneously.14
Rostral lesions were found to spread significantly more frequently to the TA and L5PS than L3/4 innervating muscles. Other investigators also demonstrated that abnormal spontaneous EMG activities were detected more frequently at the TA than at the quadriceps in ALS.34 ,35 It is noteworthy that the L5PS was also highly involved in our study. Some electromyographers claim that the paraspinalis at the lower lumbar spine may show Fib/PSWs even in healthy subjects.36 However, Fib/PSWs were not detected in normal subjects who did not have any abnormality of the lumbar spine on MRI,37 and we also selected ALS patients without lumbar spine abnormalities on MRI. The fact that the involvement was almost identical between the TA and L5PS was unexpected, although a previous report showed a similar result in the early stage of ALS,38 because LMNs of L5PS are generally considered less vulnerable than those of TA in ALS; LMNs innervating paraspinal muscles have shorter axons and smaller cell bodies than LMNs innervating distal muscles. These considerations imply a horizontal spread of ALS pathology from the more vulnerable neurons innervating the TA to the less vulnerable neurons innervating the L5PS within the L5 segment.
Another possible explanation for the frequent involvement of LMNs in the TA and L5PS is that L5 itself as a segment might be more vulnerable to ALS than other lumbosacral segments. ALS patients have lumbar spondylosis more frequently than the general population at corresponding ages,39 ,40 although lumbar spondylosis was carefully excluded in our study by detailed MRI examinations. The L5 segment accounted for 90.3% of 112 vertebrae in Japanese patients with lumbar spondylosis.40 Daily repetitive movements of the lumbar spine may cause weight-bearing biomechanical stresses particularly on L5, possibly inducing chronic minor trauma of the nerve root. Experimentally, injuries to the anterior root have been demonstrated to produce mislocalisation of TDP-43 in spinal motoneurons.41 These considerations suggest an L5 segmental vulnerability to ALS lesions, but among cervical segments, the segment C8 innervating FDI which is the most vulnerable in ALS,7 ,9 ,10 ,34 is different from the segment that is commonly affected in cervical spondylosis.42
Kiernan and his colleagues have reported that cortical hyperexcitability is an early feature in ALS, and UMN and LMN dysfunction coexists.43 We cannot take account of the influence of UMN impairments by spontaneous EMG activities we have investigated, hence we reviewed the clinical UMN features of the 14 patients who showed ‘non-contiguous pattern’ at nEMG examination (see online supplementary table S1). We can assume that they should show UMN features in both onset and lumbosacral regions if the non-contiguous pattern of nEMG is driven by the preceding UMN involvements. However, our results showed no UMN features were revealed in cervical regions in five patients (patients 23, 24, 30, 32, 35) and in lumbosacral regions in three patients (patients 24, 30, 33), neither. This result indicates the existence of some skipping mechanisms of LMN involvements regardless of UMN in propagation of ALS. On the other hand, UMN features were widespread in the rest of the patients of non-contiguous pattern. Especially, hyperreflexia was simultaneously shown in both patella tendon (quadriceps femoris; L3/4) and Achilles tendon (GC and soleus; S1) to almost the same degree even in the patients with L3/4 skipping pattern. From these findings, we could not indicate that cortical hyperexcitability is driving the non-contiguous spread of LMN involvement in ALS. However, it is well documented that cortical hyperexcitability evaluated by short intracortical inhibition with threshold tracking transcranial magnetic stimulation techniques precedes clinical UMN features,43 which is supported by the neuropathological examination that 50% of progressive muscular atrophy patients had pyramidal tract degeneration.44 Therefore, more detailed electrophysiological analysis is needed for elucidating the role of upper motor neuron dysfunction on this non-contiguous spread, because it is a potential target of therapeutic intervention, especially riluzole.45 ,46
FPs are considered to appear in the muscles which are in the earlier stage of involvement and are involved more slightly, especially the muscles which is located away from onset region, while Fib/PSWs tend to appear later than FPs and tend to appear in the onset muscle.32 ,33 ,4,7 The fact that only L5 innervating muscles in the lumbosacral regions show Fib/PSWs less rarely than FPs suggests that L5 segment is involved at first in the lumbosacral regions and then neighbouring segments are subsequently involved.
We also analysed the anatomical distribution of the involved motoneuron pools of the lumbosacral segments in the eight patients with non-contiguously affected lumbosacral lesions. The involved motoneuron pools were located in close proximity to one another horizontally or radially, appearing to form a cluster in four patients. Local propagation of pathology between motor columns can exist after the second hit in the lumbosacral cord following the first hit at the rostral onset site (see online supplementary figure S3B). If it is true, for explanation for horizontal spread between distinct motor columns, we have to assume a different mechanism from neuron-to-neuron protein transfer; for example, diffusion of a secreted toxic soluble factor or glia-to-neuron interaction which is known in the mutant SOD1 transgenic mouse4,8 may play a role in a transmission between motor columns.
In conclusion, the results of our prospective study and detailed nEMG results in 36 ALS patients showed that LMN involvement in many early stage ALS patients was distributed non-contiguously in the rostrocaudal direction of the spinal segments, indicating that the onset site is not single even with consideration of difference in motoneuronal vulnerability. On the other hand, local involvements of the anterior horn lesions tended to be formed as some clusters, and therefore, we here propose ‘multifocal hits and local propagation’ as a new hypothesis for one of the mechanisms of ALS progression.
Acknowledgments
We sincerely thank Dr Nobuo Sanjo, Hiroyuki Tomimitsu, Takuya Ohkubo, Taro Ishiguro, Akira Machida, Makoto Takahashi, Yuji Hashimoto and Masahiko Ichijo (Department of Neurology and Neurological Science, Graduate School, Tokyo Medical and Dental University); Dr Shuta Toru (Department of Neurology, Nakano General Hospital); Dr Hiroaki Yokote (Department of Neurology, Musashino Red Cross Hospital); Dr Zen Kobayashi and Yoshiyuki Numasawa (Department of Neurology, JA Toride Medical Center); Dr Masato Obayashi (Department of Neurology, National Disaster Medical Center); Dr Minoru Kotera and Yoko Ito (Department of Neurology, Tsuchiura Kyodo Hospital); Dr Kotaro Yoshioka (Department of Neurology, Yokohama City Minato Red Cross Hospital); Dr Mutsufusa Watanabe and Dr Hiroya Kuwahara (Department of Neurology, Tokyo Metropolitan Bokutoh Hospital); Dr Osamu Tao (Department of Neurology, Ome Municipal General Hospital); and Dr Kazuaki Kanai (Department of Neurology, Graduate School of Medicine, Chiba University) for their excellent technical assistance and referral of patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors TS, TK, KS, SM, SK and TY designed the study. TS, TK, KS, Y-iN, YY, AI and KA conducted the examinations. TS and TK performed statistical analysis. TS, TK and TY drafted the manuscript. SO, TK, TK, MN, HM and TY supervised the study. The version to be published was approved by all of the authors. TS accepts full responsibility for the data as the guarantor.
-
Funding This research was supported by a Grant-in-Aid for Scientific Research (A) to Yokota (#22240039); a Grant-in-Aid for Exploratory Research to Kanouchi. (#24659425); and Research on Neurodegenerative Diseases/ALS from the Ministry of Health, Labour, Welfare, Japan to Mizusawa; and Strategic Research Program for Brain Science, Field E from Ministry of Education, Culture, Sports and Technology, Japan to Mizusawa.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The local ethics committees of Tokyo Medical and Dental University School of Medicine (No. 1091), Chiba University Graduate School of Medicine (No. 769), Kyoto Prefectural University of Medicine (No. E-367), Musashino Red Cross Hospital (No. 26), Kanto Central Hospital (No. 1 of Jan 12, 2012) and Nakano General Hospital (No. 23-005) approved this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The principal investigator: Teruhiko Sekiguchi has full access to all of the patients’ clinical data including EMG results and takes full responsibility for the data, the accuracies of analyses and interpretation, and the conduct of the research.