Article Text

Abstract
Objective To evaluate the efficacy of an evidence-based patient information programme aiming to increase informed choice in patients with early multiple sclerosis (MS).
Background Patients with early MS face a number of uncertainties concerning diagnosis, prognosis and effectiveness of immunotherapy. Prior studies suggest that evidence-based patient information combined with group education can promote informed choice in MS patients.
Methods A 12-month, six-centre, double-blind randomised controlled clinical trial with 192 patients with a diagnosis of confirmed relapsing-remitting MS or clinical isolated syndrome in Germany. A 4-h interactive evidence-based educational programme was compared with a 4-h MS-specific stress management programme. The primary endpoint was informed choice after 6 months comprising risk knowledge and congruency between attitude towards immunotherapy and actual immunotherapy uptake. Secondary endpoints included autonomy preference, decision autonomy, decisional conflict and satisfaction, anxiety and depression, and number of immunotherapies.
Results For the primary endpoint, a significant difference was shown with 50 of 85 (59%) participants in the intervention group achieving informed choice after 6 months compared with 18 of 89 (20%) in the control group (OR 0.2 (95% CI 0.1 to 0.4), p<0.001). Four weeks after the intervention, more participants in the intervention group showed good risk knowledge (difference between groups 39% (95% CI 26% to 53%), p<0.001). There were no significant differences between groups for attitude towards immunotherapy and for immunotherapy uptake. There were trends towards increased autonomy preference after the intervention and increased adherence to immunotherapies in the intervention group.
Conclusions The intervention significantly increased informed choice and relevant risk knowledge without negative side effects.
- Multiple Sclerosis
Statistics from Altmetric.com
Introduction
Multiple sclerosis (MS) affects patients in a sensitive situation in life where decisions on personal life, family and professional career planning must be made. There are essential uncertainties in the current knowledge about all relevant areas of MS, that is, pathogenesis, diagnosis, prognosis and treatment.1–3 Once a diagnosis has been established, disease course and symptoms vary greatly between patients.2 ,4 ,5 Despite many efforts, only few and weak predictors for the future disease course have been proven valid.2 ,6 Parallel to revised diagnostic criteria, different disease modifying drugs (DMDs) were approved for early MS therapy. Guidelines recommend starting treatment as early as the occurrence of first symptoms, although the short-term effects remain modest and long-term data are inconclusive.7–9 Patients are now faced with an increasing number of available DMDs. High levels of anxiety and depression have been reported for patients during or soon after the MS diagnostic process.10–12 In this sensitive situation, patients often feel compelled to make decisions on drug therapy. Most available patient information materials do not mention uncertainties of available research evidence and do not discuss the option to refrain from DMDs. This is in contrast to recommendations for patient information aiming to allow for ‘informed patient choice’ and ‘shared decision making’ between patients and physicians.13 Adherence rates to MS treatments are as low as 50% with a substantial number of early terminations.14 Improving understanding and knowledge can enhance patients’ autonomy and subsequently lead to better resource use.15 Our previous studies have shown that MS patients claim active roles, appreciate comprehensive information, are able to handle risk calculation tasks16 ,17 and can cope with uncertainty.18 Solari et al19 have studied comprehensive information with additional physician-based counselling directly after an MS diagnosis, resulting in increased knowledge and satisfaction without negative side effects, but this intervention was physician-based, did not apply evidence-based patient information and did not focus early DMD decision making. In summary, there is a clear need for better patient information and decision support, especially in the diagnostic process and the early stages of MS. This study evaluates the efficacy of an evidence-based patient information programme for patients with early MS aiming to enhance informed choice and patient autonomy.
Methods
Study design
We performed a double-blind randomised controlled trial with a follow-up of 12 months using computer-generated randomisation lists for concealed allocation of participants by external central telephone. Participants were stratified by study centre and drawn consecutively using separate randomisation lists for each of the six study centres. Participants were blinded to study groups as they were not informed about the ‘active’ intervention. Outcomes were assessed via blinded telephone calls and mailed questionnaires.
Subjects
Participants were recruited between May 2009 and October 2010 at six German university-based MS out-patient clinics and followed-up for 1 year. Patients were made aware of the study by flyers and/or posters displayed at the MS centres. Also staff directly informed eligible patients attending the MS centre. At this point, no eligible patients were excluded. Patients were included if they reported a diagnosis of clinical isolated syndrome or definite relapsing-remitting MS within the last 2 years and were aged between 18 and 60 years. Patients with primary or secondary progressive MS and/or major cognitive deficits (ie, obvious inability to follow instructions) were excluded.
Interventions
Based on preparatory work and prestudies,16–18 ,20 ,21 a complex intervention was developed following an established framework.22 The intervention group (IG) received an interactive 4-h education programme, presenting the best available evidence regarding diagnostic testing in MS, prognosis of MS and early MS DMD therapy (table 1).
Components of the intervention
Two weeks before the education programme, IG participants received a 57-page educational booklet summarising relevant methodological information as well as the recent evidence on diagnosis, prognosis and early therapies in MS (available online: http://www.download.ms-netz-hamburg.de/download.php?downloadfile=PEPADIP_Final_11-11-12.pdf). Information was derived from systematic literature reviews and presented based on the principles of evidence-based patient information.23 Information on treatment options was mainly based on randomised controlled trials and trial extensions on interferon-β or glatiramer acetate. The curriculum followed the theory of planned behaviour and specifically addressed its factors, that is, attitude, normative beliefs and behavioural control.24 ,25 The programme was led by non-medical persons (JP or SaK) from the Hamburg centre and was based on structured presentation materials and moderation cards. It intended to promote informed choice rather than a specific behaviour (eg, uptake of diagnostic testing or DMD). Therefore, apart from the provision of evidence-based patient information, the programme aimed to enable participants to discuss and reflect upon the evidence and its personal relevance using different approaches, for example, small group discussions to reflect on options (table 1). To control for unspecific attention effects and enable patient blinding, control group (CG) participants took part in a 4-h MS-specific stress management programme led by a specially trained psychologist. The programme was developed by the Dresden group (SiK, TZ) based on a previously developed programme.26 The cognitive behavioural programme focuses on experience with management of stress and anxieties and aims to enhance participants’ resources as well as stress coping strategies. Two weeks before the programme, patients in the CG received a short 5-page information leaflet with information on diagnosis, prognosis and early therapy as provided on the website of the German MS society (http://www.dmsg.de).
Outcome measures
Informed choice
The primary endpoint was the proportion of participants displaying ‘informed choice’ after 6 months of follow-up assessed using the validated ‘Multi-Dimensional Measure of Informed Choice’27 adapted to early MS. Following the instrument, DMD choices were classified as 'informed’ or ‘uninformed’, according to participants’ relevant risk knowledge, their attitude to take or not to take a DMD, and DMD status. The instrument defines ‘informed choice’ as congruency between attitude and uptake combined with good risk knowledge. Therefore, participants with good risk knowledge and a positive attitude who were on a DMD after 6-month were classified as making an informed choice. Also, participants with good risk knowledge and a negative attitude who were not on a DMD were classified as making an informed choice. Risk knowledge was assessed 2 weeks after the intervention using an adapted 19-item multiple choice questionnaire based on earlier work.16 The original questionnaire had been restructured based on a survey with 77 MS patients using 197 risk knowledge questions. Based on these data, the former questionnaire was adapted for recently diagnosed patients and piloted with 34 MS patients showing satisfactory psychometric results. In this study, the cut-off value for ‘good knowledge’ had been defined a priori as the value that 30% of all participants reached at baseline in the total study population, that is, 12 or more of 19 possible correct answers. Attitude towards DMDs was assessed using a single question 2 weeks after the intervention. Uptake was defined as self-reported DMD status 6 months after the intervention. We applied this time-frame to allow for sufficient time for decisional processes to evolve.
DMD status
Participants were asked before randomisation and at 3, 6, 9 and 12 months about their current DMD status during a telephone interview.
Autonomy preferences
The Control Preference Scale28 was used to assess autonomy preferences 2 weeks before, 2 weeks and 12 months after the intervention. The scale provides five descriptions of role distributions in physician–patient interactions ranging from ‘autonomous’ to ‘paternalistic’ roles with ‘shared decision making’ representing the neutral category. As carried out in a previous trial,29 participants received the descriptions printed on cards and were asked to sort the cards following their preference hierarchy. For analyses, only the first choice, that is, the top card was used.
Decision autonomy and satisfaction
Decision autonomy was assessed in patients who reported a decision on DMD during the 3 months preceding the telephone interviews at 3, 6, 9 and 12 months. Following the decision roles outlined in the Control Preference Scale, patients were asked to apply five possible roles to the actual decision. Also for each decision, satisfaction with the decision was assessed using three possible answers.20 ,29
Decisional conflict
We used the German version of the Decisional Conflict Scale30 comprising of five subscales (uncertainty, informed, values clarity, support, effective decision). We applied the Decisional Conflict Scale 2 weeks before the intervention and after 12 months.
Anxiety and depression
The German version of the Hospital Anxiety and Depression31 was used before randomisation, 2 weeks and 12 months after the intervention. The scale comprises 14 items (seven for each subscale) measured on 4-point Likert scales with each item scoring 0–3 with higher values indicating increased anxiety and depression.
Decision making process
In addition to assessing attitude (ie, intention to use a DMD) with a single question, we more deeply evaluated the decision processes using the newly developed and recently validated ‘Planned Behaviour in MS’ (PBMS) questionnaire25 2 weeks before the intervention as well as 2 weeks, 6 and 12 months after the intervention. The instrument is based on the theory of planned behaviour24 postulating three independent domains determining a certain behaviour and the intention to perform this behaviour: ‘attitude’, ‘subjective social norm’ and ‘perceived behaviour control’. As a general rule, the more favourable attitude and subjective norm and the higher perceived behavioural control, the stronger is the intention to perform the behaviour under consideration, that is, DMD therapy. The questionnaire comprises 30 items scored on a 4-point Likert scale (‘disagree’ to ‘agree’). Mean scores were calculated for all three domains (range 0–9).
Safety
Participants’ disease-related quality of life was measured before randomisation and after 12 months using the ‘Hamburg Quality of Life Questionnaire in Multiple Sclerosis.32 Participants’ disability status was assessed with a patient-based version of the UK Neurological Disability Scale before randomisation and at the end of follow-up.
Sample size
Sample size was calculated on the basis of the primary outcome measure (proportion of participants with informed choice). Based on prior studies,16 ,18 ,29 we expected 50% of IG patients to make informed decisions compared with 25% patients in the CG. In order to detect this difference with a power of 90% and a significance level of p<0.05, 85 patients per group were needed. Assuming a drop-out rate of 10%, a total of 190 participants (95 per group) were needed.
Statistical analysis
All statistical analyses were carried out using R 2.15.1. Primary comparisons assessed the effects of the intervention on an intention-to-treat-basis. For the primary endpoint ‘informed choice’, logistic regression analysis was used. Continuous data were described using means and SDs and compared using Student t test. Categorical data were presented using contingency tables and raw percentages and were compared using Fisher's exact test. Proportional odds logistic regression models were used for ordinal data such as decision autonomy. Differences between proportions were tested using Yates’ continuity correction.
Ethical issues and study registration
The study was approved by the ethics committee of the Hamburg chamber of physicians (Ref. PV3164) as the leading ethics committee as well as by all local ethic committees. All participants gave written informed consent.
The study outline was published in the ISRCTN register (http://www.controlled-trials.com/ISRCTN12440282).
Results
Participant flow and follow-up
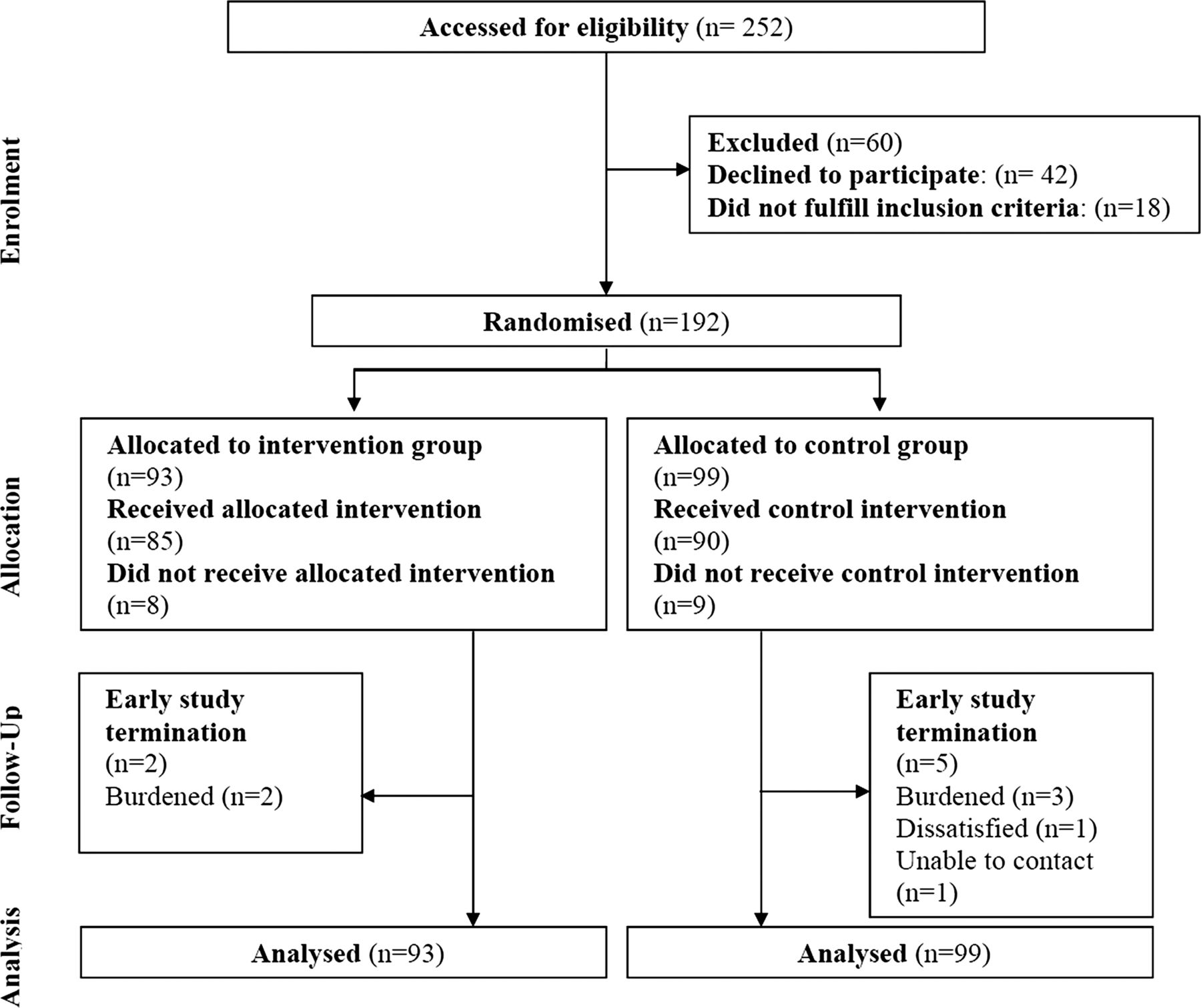
A total of 192 patients were randomised, 93 to the IG and 99 to the CG. Eight participants in the IG and nine participants in the CG did not receive the intervention due to personal time constraints (figure 1). Baseline demographics were similar between groups (table 2). Results from the cognitive items of the quality of life and the disability assessment indicate few participants with important cognitive impairment with no differences between groups (data not shown).
Baseline data
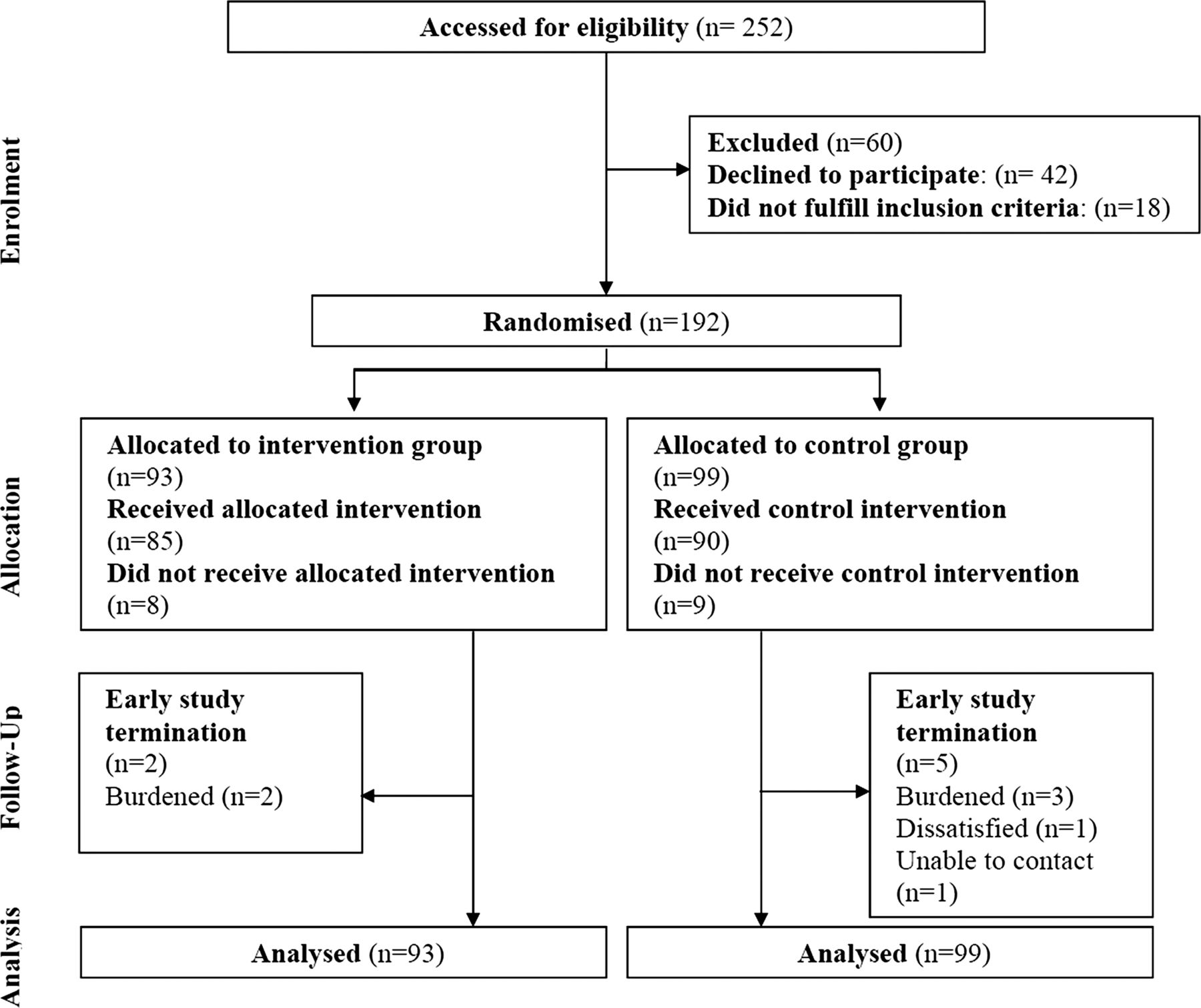
Flow of participants through the trial.
Primary endpoint: informed choice
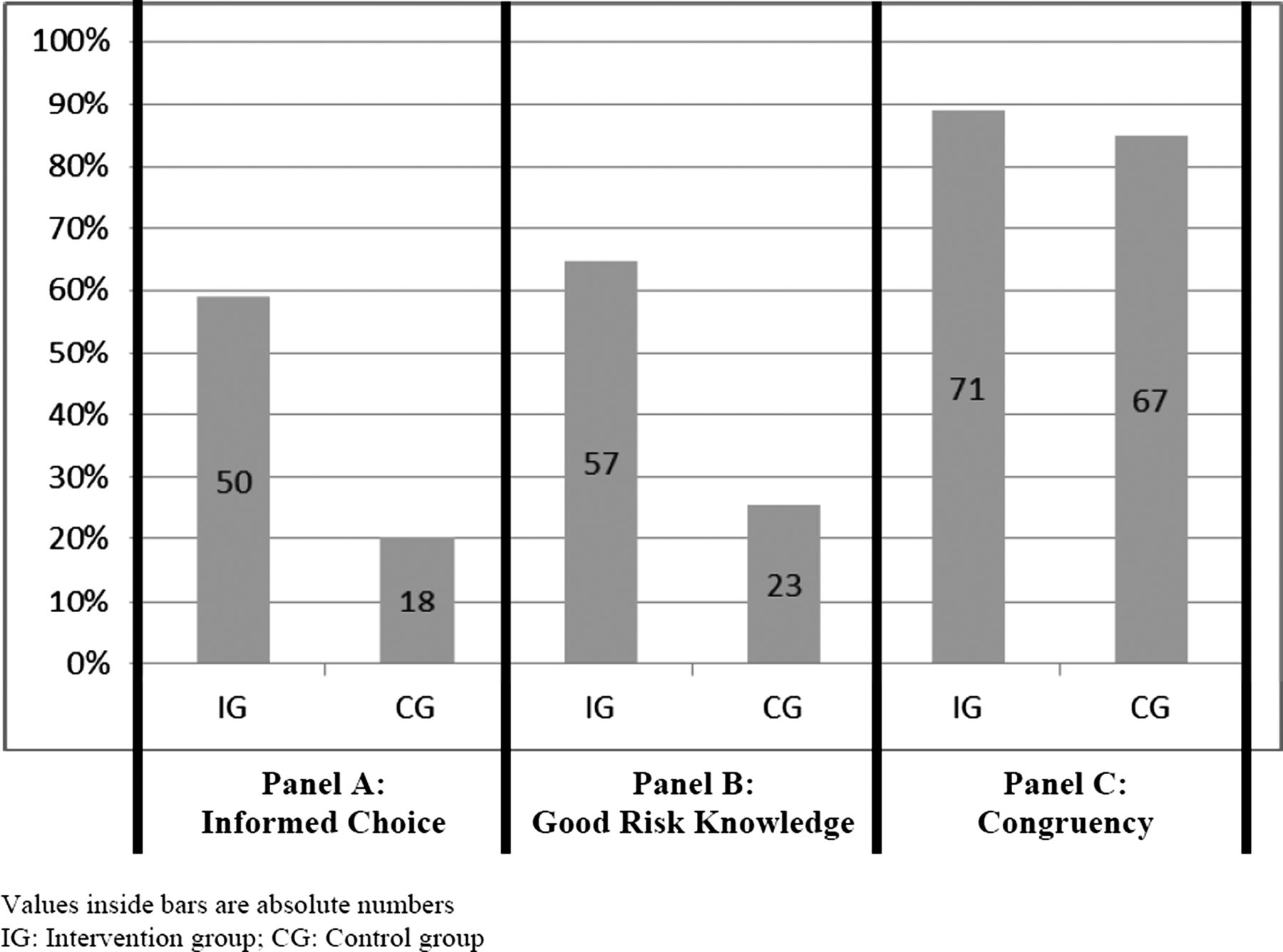
The intervention led to significantly more participants with informed choice during 6 months of follow-up (figure 2A), with 50 participants (58.8%) in the IG compared with 18 (20.2%) in the CG (difference 38.6% (95% CI 24.1% to 53.1%); OR 0.18 (95% CI 0.09 to 0.35), p<0.001). This difference was largely based on the difference in risk knowledge between groups (table 3; figure 2B) with no significant difference for attitude towards DMDs 2 weeks after the intervention (difference −0.5% (95% CI −15.1% to 14.2%), p=0.92). The same applies to congruency of attitude and uptake (figure 2C) (difference 4.0% (95% CI −6.6% to 14.5%), p=0.46).
Risk knowledge 2 weeks after intervention

{kind=link}
{kind=link}
Percentages of participants with informed choice (primary endpoint) (A), good risk knowledge (B) and congruency of attitude and uptake (C).
DMD adherence
Of those patients without a DMD at baseline, in the CG more patients newly initiated a DMD during 12-month of follow-up and of those already on DMDs, more patients discontinued DMDs although these differences were not statistically significant (table 4).
Disease modifying drug (DMD) status during follow-up
Autonomy preferences, decision autonomy and satisfaction
Overall, autonomy preferences were high with more than two-thirds preferring roles more autonomous than shared decision making (table 5). These did not differ between groups and between measurement points with a trend towards greater autonomy preference in the IG 2 weeks after the intervention (p=0.07).
Autonomy preferences (Control Preference Scale)
Overall, 70 (IG) and 72 (CG) decisions on DMDs were reported during the 12 months of follow-up. In both groups, most decisions were reported to be solely or mostly driven by the patient or were shared between patients and physicians with no differences between groups. In both groups, almost all decisions were reported as satisfactorily (data not shown).
Decisional conflict
Decisional conflict scores were low for all subgroup categories with no differences between groups neither before the intervention nor after 12 months (data not shown). Overall, values further decreased during the study for both groups.
Anxiety and depression
Mean scores of anxiety and depression were low and no significant differences between groups and between measurement points were found for Hospital Anxiety and Depression Scale assessments. At baseline, results were 7±3.6 (IG) and 7±3.7 (CG) for anxiety and 4.1±3.8 (IG) and 4.8±4.1 (CG) for depression. After 12 months, results were 6.6±3.6 (IG) and 6.8±4.1 (CG) for anxiety and 3.8±3.4 (IG) and 4.5±4.1 (CG) for depression, indicating that neither intervention had an influence on participants’ anxiety and depression levels.
Decision making process
Compared with the CG, IG participants were significantly more critical towards DMDs directly after the intervention (p=0.04) (table 6). This effect was based on more critical beliefs about what can be expected from DMDs and by a more critical attitude towards DMDs. Also, IG participants were less willing to comply with subjective social norm leading to significantly less pressure towards DMD uptake by subjective social norm (p=0.006). These effects only sustained until 2 weeks after the intervention.
Decision making process (planned behaviour in MS questionnaire)
Safety: quality of life and disability status
We found no differences in changes of health-related quality of life or disability status between groups (data not shown). Together with the results on anxiety and depression, this suggests that the programme has no negative side effect.
Discussion
The results of this double-blind randomised controlled trial show that an evidence-based patient information programme for patients with early MS, addressing many uncertainties, increases informed choice without negative side effects compared with a stress management programme. Despite high levels of autonomy in both groups, there was a trend towards increased autonomy preference in the IG directly after the intervention. At the same time point, the indepth analysis of internal reasoning regarding decisions about DMDs (assessed with the PBMS questionnaire)25 indicated less impact of social norm and more critical attitudes regarding DMDs in the IG. Also, while the proportion of patients with DMDs did not differ between groups, results indicated non-significantly higher adherence rates in IG patients. The fact that behavioural differences were only observed in the short-term may not be surprising considering the single 4-h programme. Another reason might be the intervention's lack of adapting to individual needs on the timing of a decision.
Although cognitive deficits might impact on learning abilities and decision competencies in MS, the intervention resulted in a substantial knowledge increase, indicating participants’ sufficient cognitive capacity in general.
As the intervention was applied in patients from different areas throughout Germany, generalisability of the results seems given although external validity might be limited by recruitment through academic centres. As in previous studies, we cannot exclude that particularly patients with active coping patterns participated. However, compared with an earlier more selective study,29 autonomy preferences were less marked, indicating a more representative cohort.
The best method to assess patient involvement remains unclear. The chosen Multi-Dimensional Measure of Informed Choice instrument is strongly based on knowledge, an important prerequisite which needs integration of reflection of preferences and values leading to a certain decision and a subsequent behaviour. However, the knowledge questionnaire was not directly based on the programme's content but on a former scale which was redesigned after several validation steps. Other efforts to operationalise and measure patient involvement using psychological measures have yielded little success. Especially rating scales might be strongly influenced by social desirability and self-perception.33 We have shown earlier that perceived and performed engagement in decision making on MS immunotherapies do not correlate.34 Here further research on integrating perspectives of patients, physicians as well as their integrated dyadic competence is indicated. The same holds true for the assessment of decision quality. As observed before, assessment of satisfaction with treatment decisions is associated with a pronounced ceiling effect.20
In contrast to other studies,11 in this trial only moderate to low levels of depression and anxiety as well as low levels of decisional conflict were detected. In addition, patients reported high autonomy preferences, indicating a possible selection of emotionally more stable and autonomous patients. So far, there has been no study rigorously assessing the efficacy of evidence-based patient information for patients with early MS. The study by Solari et al19 did not offer evidence-based patient information. In contrast to a previous study on DMD decision making,29 the actual study included a group session in addition to a printed information brochure to allow participants to discuss and reflect the contents of the programme. Post-trial interview and focus group data (not shown) together with experience from earlier trials indicate that the group experience was regarded important in both groups, while only the evidence-based patient information intervention was considered as relevant to deal with uncertainty and support decision making. However, as inherent in complex interventions, it remains unclear which of the intervention components contributed most to the study effect.22
While we could show altered health behaviour in the programme on relapse management,20 no significant differences in health behaviour were observed in this study. As the decision process regarding DMD treatment strongly differs from deciding on relapse treatment, a 4-h education intervention might not sufficiently empower patients to show different behaviours toward treatments. The observed trend towards higher adherence rates in the IG indicates that communicating scientific uncertainties does not simply lead to less use of DMDs, but on the contrary may induce a higher level of elaboration towards treatment, probably leading to more decisions based on patients’ preferences. This is in line with the recent call by Mulley et al35 for higher sensitivity towards patients’ preferences in medicine.
Informed choice is an ethical prerequisite for healthcare decision making. This study shows that evidence-based patient information can result in high rates of patients performing informed choice without negative side-effects. Although clinicians at least in the context of MS frequently express concern that evidence-based patient information and patient empowerment might lead to fewer patients opting for effective therapies, our results give no indication for this.
Acknowledgments
We thank the research assistants Imke Backhus, Anna Marques, Marina Tiede, Anne Rahn and Mirja Röwekamp as well as Melanie Hausdorf for providing the control intervention. We also thank the participating study centres and the study nurses and physicians at the centres in Berlin (Franziska Lipske), Giessen (Sabine Vogel), Regensburg (Ulrike Gleixner), Dresden (Raimar Kempcke) and Münster (Tilmann Graf).
References
Footnotes
-
Contributors SaK (principal investigator) together with CH and JK designed the study and protocol, together with KF, JP, JK and CH led the development of the EBPI programme, together with EV, JK and CH analysed data, interpreted results and wrote the article with important contribution from CH. SaK is the guarantor. SiK and TZ provided the stress management programme. EV performed the statistical analysis and wrote the statistical part of the article. TZ, MB, IK, MM, FP and CH provided clinical expertise. All authors contributed to the interpretation of study results and writing of the article.
-
Funding The study was funded by a grant from Merck Serono Germany. SaK was funded by the National MS Society (USA) through a research grant (rehabilitation fellowship). The funder approved the design of the study, but had no role in the conduct of the study; in the collection, management, analysis and interpretation of the data; or in the preparation, review or approval of the manuscript.
-
Competing interests JP received travel reimbursements and speaker honoraria from Bayer Healthcare. SiK received speaker honoraria from Biogen Idec, Merck Serono, Novartis and Teva. TZ received personal compensation from Biogen Idec, Bayer, Novartis, Sanofi, Teva and Synthon for consulting services and financial support for research activities from Bayer Healthcare, Biogen Idec, Novartis, Teva and Sanofi Aventis. MB received speaker honoraria from Bayer Healthcare, Biogen Idec, Merck Serono, Novartis, Sanofi Aventis and Teva and received research support from Bayer Healthcare, Biogen Idec, Merck Serono, Novartis and Teva. IK received travel reimbursements and speaker and consulting honoraria from Bayer Healthcare, Biogen Idec, Merck Serono and Novartis and research support from Bayer Healthcare, Novartis and Biogen-Idec. MM received travel reimbursements, speaker and consulting honoraria from Bayer Healthcare, Biogen Idec, Merck Serono, Novartis, Sanofi-Aventis and Teva and research support from Bayer Healthcare, Biogen-Idec, Merck Serono and Novartis. FP is a member of the advisory board of Novartis. Also, he received speaker honoraria, travel grants and research grants from Teva, Sanofi-Aventis, Bayer Schering, Biogen Idec, Merck Serono and Novartis. CH received speaker honoraria, travel reimbursements and research grants from Bayer Healthcare, Biogen Idec, Merck Serono, Teva and Novartis.
-
Ethics approval Ethics committee of the Hamburg Chamber of Physicians (Ref. PV3164) as well as all local ethic committees.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Requests for data sharing should be directed to SaK and would be considered as required.