Article Text

Abstract
Objective Chromosome 1p/19q deletion is an established prognostic and predictive marker in the WHO grade III oligodendroglial tumours (OT). To estimate the genetic status preoperatively, the authors investigated the correlation between the uptake of 11C-methionine in positron emission tomography (PET) and the 1p/19q status in grades II and III OT.
Methods We retrospectively reviewed 144 patients with gliomas who received 11C-methionine PET. 66 cases with grades II–III oligodendrogliomas or oligoastrocytomas underwent fluorescence in situ hybridisation to determine the 1p/19q status. The tissue uptake of 11C-methionine was expressed as the ratio of the maximum standardised uptake value (SUVmax) in tumour areas to the mean SUV (SUVmean) in the contralateral normal brain (tumour-to-normal tissue (T/N) ratio).
Results The T/N ratio in 11C-methionine PET was significantly higher in grade III OT than in grade II tumours. The mean T/N ratio of the grade II tumours without 1p/19q deletion was significantly higher than that of the grade II tumours with 1p/19q deletion (mean 2.67 vs 1.94, respectively; p=0.0457). In grade III tumours, the mean T/N ratio of the tumours without 1p/19q deletion was also significantly higher than that of the tumours with 1p/19q deletion (mean 4.83 vs 3.49, respectively; p=0.0261). The rate of IDH1 mutation was lower and the rate of contrast enhancement on MRIs was higher in the 1p/19q non-deleted OT than those with 1p/19q deletion, which may contribute to the high T/N ratio.
Conclusions Among suspected OT, 11C-methionine PET may help us preoperatively discriminate tumours with and without 1p/19q deletion.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Gliomas are the most common primary brain tumour in adults. Since gliomas arise in the brain in which there is a functional localisation, the tumours usually cannot be resected completely. On the basis of their morphological appearance, gliomas can be classified into two major subtypes: astrocytic tumours and oligodendroglial tumours (OT) including mixed oligoastrocytic tumours.1 Astrocytic tumours are usually refractory to radiotherapy and chemotherapy, and frequently progress to the more malignant grades. On the other hand, OT is sensitive to these treatments and is associated with better patient survival.2–5 The histological classification of tumour subtype and grade is thus important for guiding treatment decisions.
To date, three important prognostic markers for gliomas have been identified: chromosome 1p/19q deletion,6 methylation in the promoter region of O6-methylguanine-DNA methyltransferase (MGMT) gene,7 and isocitrate dehydrogenase (IDH) gene mutation.8 Among them, only 1p/19q deletion is both a prognostic and predictive marker in grade III OT.9 ,10 Furthermore, this chromosomal aberration indicates the presence of an oligodendroglial component, and serves as a diagnostic hallmark of OT.5 ,11 If clinicians were able to obtain specific biological information preoperatively, an optimal treatment strategy could be determined better than with conventional imaging modalities alone.
Molecular and physiological imaging techniques show promise for the non-invasive and preoperative characterisation of glioma biology.12 Positron emission tomography (PET) with 18F-fluorodeoxyglucose (FDG) and 11C-methionine is frequently used to obtain diagnostic and prognostic information, to guide appropriate biopsy, to distinguish tumour recurrence from radiation necrosis, and to monitor therapy response in gliomas as well as primary central nervous system lymphoma and meningioma.13–16 Recently, the authors reported that 11C-methionine PET can distinguish low-grade gliomas from high-grade gliomas, and may help discriminate low-grade OT from diffuse astrocytomas.17 Since uptake of the tracer 11C-methionine is generally higher in OT than in astrocytomas of the same grade, 11C-methionine PET imaging may be useful for detecting the biological characteristics of OT including the status of 1p/19q.
To evaluate the ability of 11C-methionine PET to detect the biological features resulting from the 1p/19q deletion, we analysed correlations between the quantitative results of 11C-methionine PET and histological classification, Ki-67 labelling index, contrast enhancement on MRI, IDH1 status, and 1p/19q status in patients with OT.
Methods
Patients
A total of 144 patients with histologically confirmed gliomas underwent 11C-methionine PET at the National Institute for Radiological Science (NIRS) or at Chiba Medical Center for Prolonged Traumatic Brain Dysfunction between 2002 and 2014 (table 1). Their medical records were reviewed retrospectively. An analysis of the first half of the cohort (70 cases) has been reported previously,17 and an independent analysis of the second half of the cohort was also performed. Institutional Review Board approval for the study protocol was obtained. Each patient was required to provide written informed consent. We performed maximum possible resection of the tumour including the area with the highest 11C-methionine uptake. In case such a maximum resection was not possible, the highest uptake portion was sampled with the guidance of a navigation system. All tumour samples were histologically diagnosed according to the WHO classifications: grade I gliomas in 10 cases, diffuse astrocytoma in 18 cases, anaplastic astrocytoma in 17 cases, OT in 37 cases, anaplastic OT in 29 cases and glioblastoma in 33 cases. The group included 97 men and 47 women, and the mean age was 45 years (range 16–77 years). Fifty-eight (40%) had total resection and 86 (60%) had partial resection. All patients underwent surgical procedures within 2 weeks after PET.
T/N ratios of methionine SUV, IDH1 gene status, and contrast enhancement by tumour type and grade
Methionine PET
11C-methionine PET was done with a high-resolution full-ring scanner (Biograph; Siemens/CTI or Discovery ST-E; GE Healthcare). Details are described in our previous report.16 PET images were acquired in a resting state after fasting for ≥4 h. Static scanning was done for 6 min with three-dimensional (3D) acquisition, and images were reconstructed with a 3D ordered-subset expectation maximisation algorithm. CT-based attenuation-corrected PET images were employed with Discovery ST-E. 11C-methionine was administered intravenously in a dose of 370–720 MBq, and the scan began 20 min after injection. Summation images covering 20–40 min after administration were used for analyses. Accurate co-registration of CT and PET images was obtained with commercially available software (Advantage Workstation; GE Healthcare).
A circular region of interest (ROI) 10 mm in diameter was set in the hot spot of each tumour. Tracer accumulation in the ROI was represented as a standardised uptake value (SUV), which shows the activity concentration in the ROI divided by the injected dose normalised to the body weight of the patient. We also set five ROIs in the contralateral normal brain region to calculate the average. The methionine tumour-to-normal tissue (T/N) ratios were calculated as the ratio of the maximum SUV of the tumour (T) to the mean SUV of the contralateral normal brain (N), and used for evaluation of the diagnostic efficacy of methionine PET.
MRI study
MRIs were obtained on a 1.5 or 3.0 T system (Signa; GE Medical System, Milwaukee, Wisconsin, USA). In addition to the T1-weighted and T2-weighted axial images without contrast enhancement, the contrast-enhanced T1-weighted axial images were obtained after injection of 0.2 mL/kg gadopentate dimeglumine. The parameters used for MRI were as follows: 5.0 mm thickness, gap 1 mm, repetition time (TR)/echo time (TE)=400/20.0 ms, NEX=1).
Analysis of 1p/19q deletion
A standard fluorescence in situ hybridisation (FISH) was done on a fixed cytogenetic preparation from fresh tumour tissues to determine the 1p/19q status. FISH probes for chromosome 1p were the target region of 1p36 with a control region of 1q25, and those for chromosome 19q were the target region of 19q13 with a control region of 19p13. Signals were separately counted and scored, and a ratio of 1p:1q or 19q:19p of <0.75 was diagnosed as loss. Loss of only 1p or only 19q was not regarded as a tumour with a deletion because this type of chromosomal abnormality is non-specific and observed in many other tumours.
Histopathological and immunohistochemical analyses
Formalin-fixed, paraffin-embedded surgical specimens were stained with H&E, which were used for histological classification and analysis of cell density. Cell counting was done under a light microscope at ×200 magnification and represented as the number of cells/mm2. Data were recorded as the mean of three different portions of the specimens. The target antigens were retrieved by autoclaving prior to immunohistochemistry. The samples were incubated with the antibody overnight. The primary antibodies were MIB-1 monoclonal antibody for Ki-67 antigen (Immunotech, Westbrook, ME) and antihuman IDH1-R132H monoclonal antibody (IBL Co, Ltd, Gunma, Japan) according to the manufacturer's recommendation using commercially available reagents. Sections were then incubated with the biotinylated secondary antibody (1:500, DAKO, Tokyo, Japan) in the same buffer. The bound antibodies were visualised with the avidin-biotin peroxidase complex method and diaminobenzidine tetrachloride. For scoring positive rates, 1000 tumour cell nuclei were counted in ×200 fields, and the labelling index was expressed as the per cent of labelled tumour cells. This evaluation was performed in a blinded manner without knowledge of the patient outcome. To evaluate IDH1 staining, strong cytoplasmic staining in any number of cells was scored as positive.
Statistical analyses
Differences in SUV T/N ratios among different groups of gliomas were examined with one-way analysis of variance. The unpaired t test and χ2 test were used to analyse the correlation between two different groups. The receiver operating characteristics (ROC) curve analysis was used to determine the optimal cut-off values for the differential diagnosis of tumours with and without 1p/19q deletion. These statistical analyses were done by using Stat-View software and SAS software (SAS Institute Inc, Cary, North Carolina, USA).
Results
Correlation between the T/N ratio and tumour type, grade and IDH1 genotype
The SUV T/N ratios in 11C-methionine PET vary among tumour types, grades and 1p/19q genotypes. We validated our previous findings that the T/N ratio is greater in higher grade tumours than in lower grade tumours, as well as in OT than in astrocytic tumours (table 1).17 The mean T/N ratio in diffuse astrocytomas was 1.06, and many cases showed values less than 1, which clearly shows that 11C-methionine PET cannot precisely delineate the tumour areas of diffuse astrocytomas.
In OT, the SUV T/N ratios obtained with 11C-methionine PET were 2.33±0.82 (mean±SD) for grade II tumours and 4.01±1.47 for grade III tumours. The mean T/N ratio was higher in grade III OT than in grade II tumours (p<0.0001).
Over 80% of the cases had mutated IDH1 in grades II and III gliomas except for grade III anaplastic OT without 1p/19q deletion and glioblastoma. In particular, most of grade II OT both with and without 1p/19q deletion had IDH1 mutation. In contrast, only 17% of glioblastoma had the mutation. In grade III tumours, the ratio of IDH1 mutation in anaplastic OT without 1p/19q deletion was 40%, whereas that in the tumours with 1p/19q deletion was 87% (p=0.0143; table 1).
T/N ratio and 1p19q deletion in OT
The 1p/19q deletion was observed in 44 of 66 cases of OT (67%), including 26 of 37 cases (70%) of grade II tumours and 18 of 29 cases (62%) of grade III tumours. OT without 1p/19q deletion had a significantly higher T/N ratio (3.26±1.00) than those with 1p/19q deletion (2.52±1.13; p=0.0290). We then performed a separate analysis according to the WHO histological grade. In grade II OT, the mean T/N ratio was 1.94±0.58 for tumours with 1p/19q deletion and 2.54±0.43 for tumours without the deletion (p=0.0457) (figure 1). In grade III tumours, the mean T/N ratio was 3.49±0.84 for tumours with the 1p/19q deletion and 4.83±1.37 for those without 1p/19q deletion (p=0.0261). Thus, OT without 1p/19q deletion had significantly higher 11C-methionine PET T/N ratios than those with 1p/19q deletion in grades II and III tumors (figure 2). The ROC curve analysis showed that a cut-off T/N ratio of 2.54 for grade II tumours and 4.47 for grade III tumours provided the best sensitivity and specificity to determine 1p/19q status in the present cohort (sensitivity of 88% and specificity of 64% in grade II tumours, and sensitivity of 83% and specificity of 64% in grade III tumours). When the analysis was limited to the second half of the cohort, the result was robust and showed that the T/N ratio was significantly higher in the 1p/19q non-deleted tumours than in the tumours with the deletion in both grades (p=0.0028 for grade II and 0.0143 for grade III).

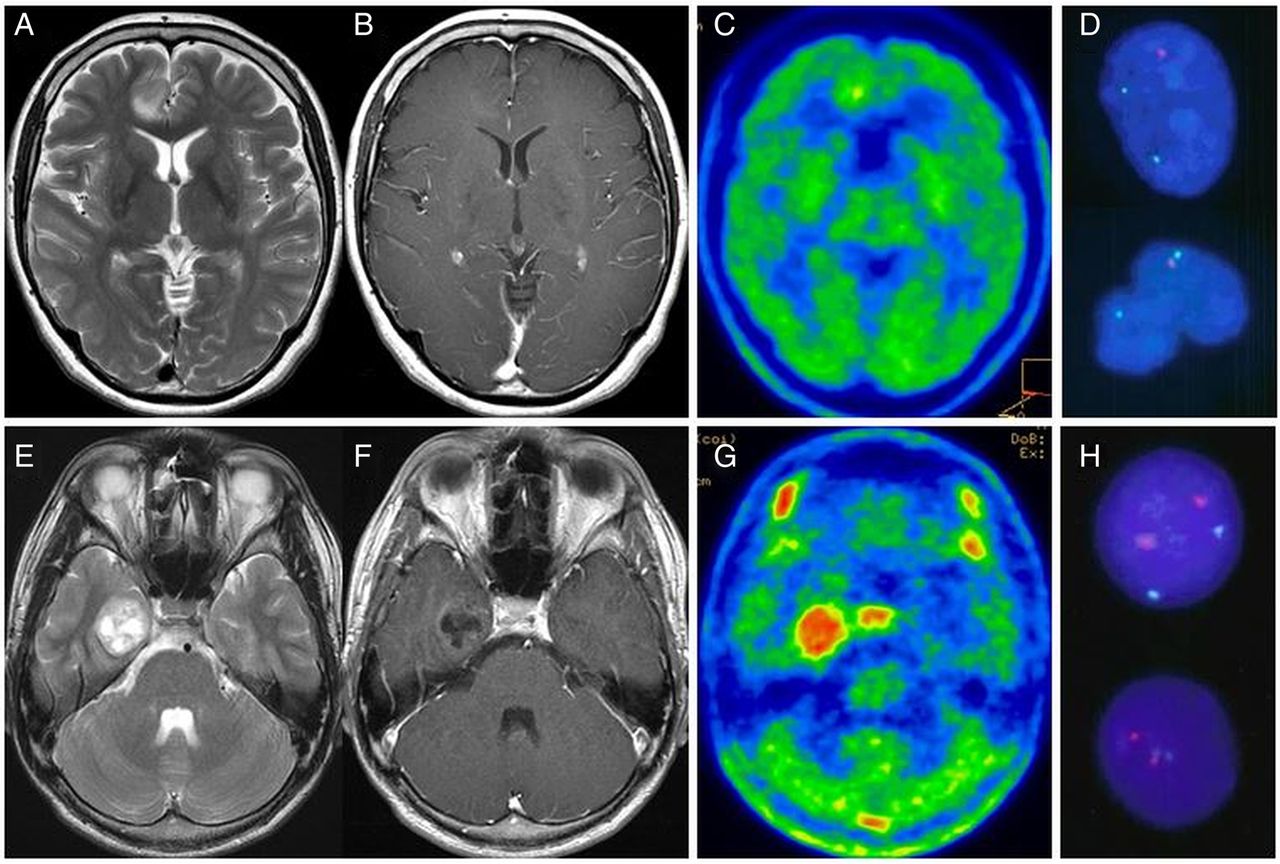
Representative images from patients with grade II oligodendroglioma with 1p/19q deletion (upper panels: (A) T2-weighted MRI, (B) gadolinium (Gd)-enhanced T1-weighted image, (C) methionine positron emission tomography, (D) fluorescence in situ hybridisation (FISH) for 1p/19q status), and grade II oligodendroglioma without 1p/19q deletion (lower panels: (E) T2-weighted MRI, (F) Gd-enhanced T1-weighted image, (G) methionine PET, (H) FISH for 1p/19q status).

Bar graphs of methionine standard uptake values (SUV) for tumour-to-normal tissue (T/N) ratios comparing various subtypes of oligodendroglial tumours and glioblastoma; (A) grade II oligodendroglial tumours with 1p/19q deletion (n=26), (B) grade II oligodendroglial tumours without 1p/19q deletion (n=11), (C) grade III oligodendroglial tumours with 1p/19q deletion (n=18), (D) grade III oligodendroglial tumours without 1p/19q deletion (n=11), (E) glioblastoma (n=33). In grades II and III, the T/N ratio is significantly higher in tumours without 1p/19q deletion than in tumours with the deletion (p=0.0457 and 0.0261, respectively).
Cell density, Ki-67 index and contrast enhancement on MRI
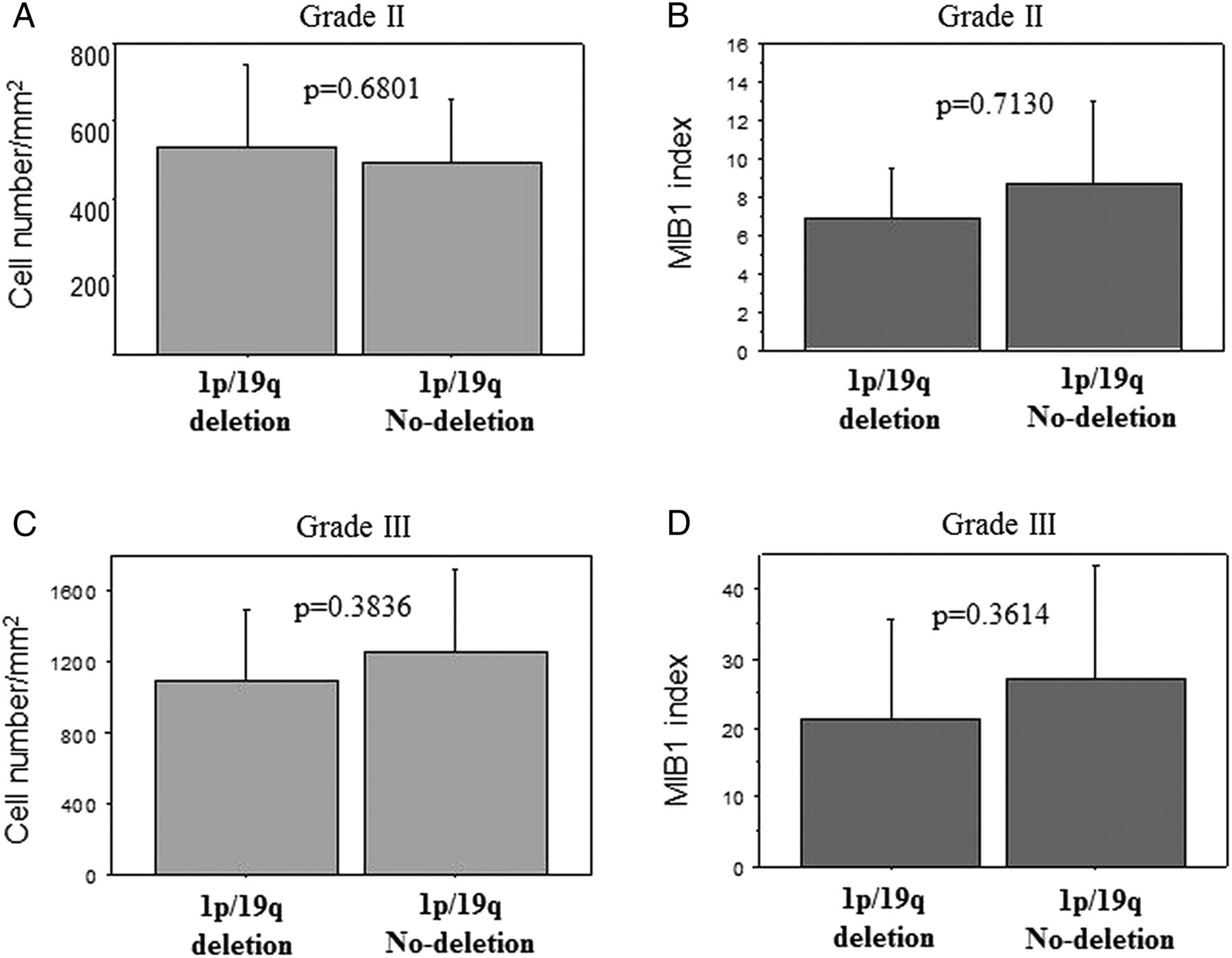
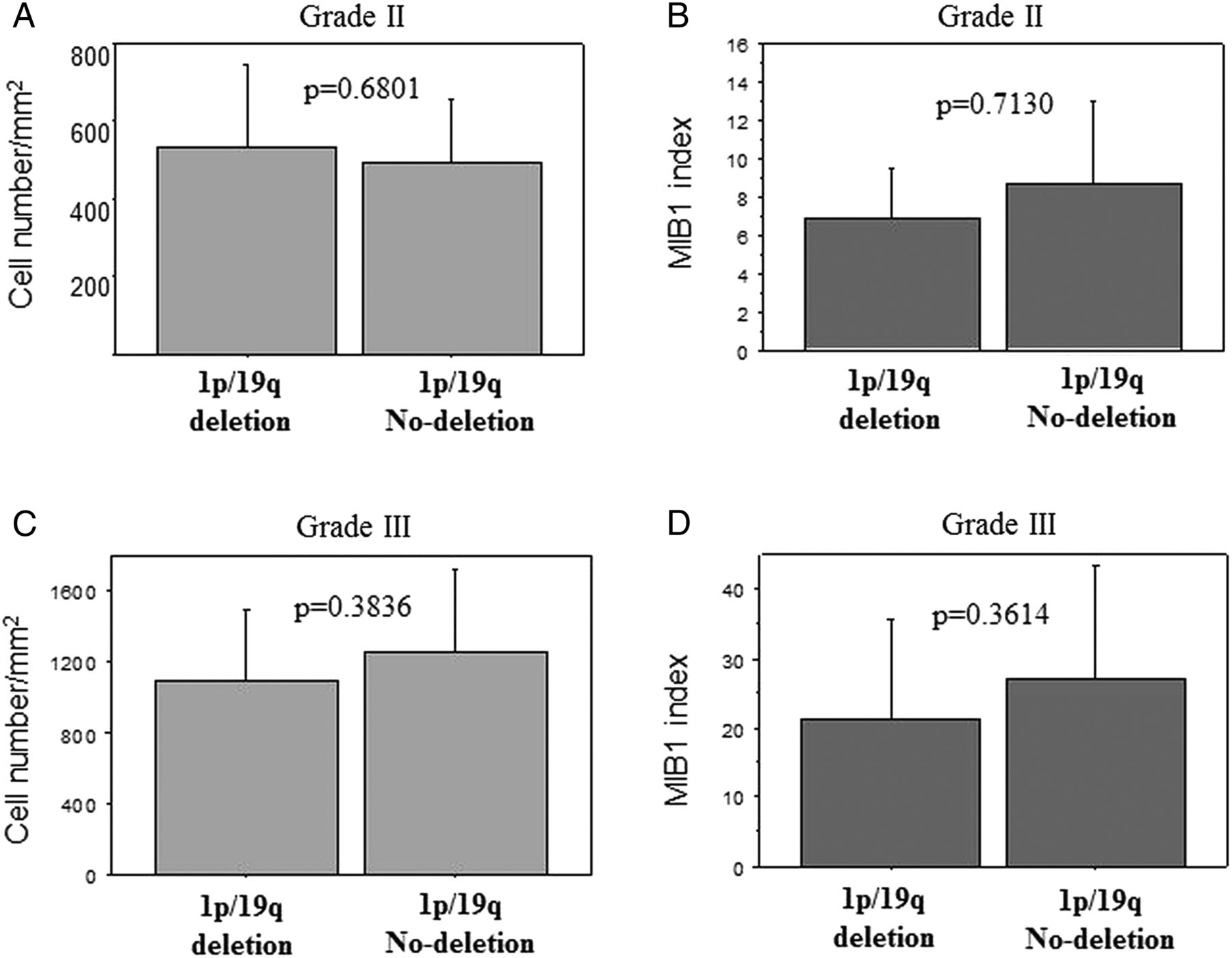
To assess a possible explanation for the differences in the 11C-methionine PET T/N ratio, cell density and Ki-67 labelling index were compared in tumours with and without 1p/19q deletion. We found no significant differences between tumours with and without 1p/19q deletion for either cell density or Ki-67 labelling index both in grades II and III tumours (figure 3). The Ki-67 index was approximately four times higher in grade III tumours than in grade II tumours, and tended to be higher in the 1p/19q non-deleted tumours than in the deleted tumours without statistical significance.
{kind=link}
{kind=link}
{kind=link}
Bar graphs comparing cell density (A) and the Ki-67 labelling index (B) between oligodendroglial tumours with 1p/19q deletion and those without. In both categories, no significant differences were found depending on the 1p/19q status. Upper panels: grade II oligodendroglial tumours, lower panels: grade III oligodendroglial tumours.
Contrast enhancement on MRI is a candidate parameter of metabolic activity. Grade III OT without 1p/19q deletion were significantly associated with a higher rate of contrast enhancement on MRI (p=0.0094). Grade II tumours without 1p/19q deletion also tended to have a higher rate of contrast enhancement on MRI, but the difference did not reach statistical significance (p=0.078).
Discrimination between grade III OT and glioblastoma
Discrimination of grade III OT from the WHO grade IV glioblastoma is clinically important for adequate surgical planning because the clinical courses of these two tumour types are quite different. Although the mean T/N ratio of grade III tumours without 1p/19q deletion (4.83±1.37) was not different from that of glioblastoma (the mean T/N ratio was 4.25±1.59, p=0.3607), that for grade III tumours with 1p/19q deletion was significantly lower than glioblastoma (the mean T/N ratio was 3.49±0.84, p=0.0258). This result suggests that grade III OT with 1p/19q deletion, which usually have a better prognosis than glioblastoma, can be preoperatively predicted with 11C-methionine PET. To discriminate grade III OT with 1p/19q deletion from glioblastoma or those without 1p/19q deletion, the ROC curve analysis showed that a cut-off T/N ratio of 3.63 provided the best sensitivity and specificity in the present cohort (sensitivity of 67% and specificity of 70%).
Discussion
The present study clearly showed that the mean SUV T/N ratio obtained with 11C-methionine PET was significantly higher in OT without 1p/19q deletion than in those with this chromosomal aberration. The T/N ratio cut-off values of 2.54 for grade II tumours and 3.63 for grade III tumours will be important in daily clinical practice, in combination with other imaging modalities to predict tumour grade. In tumours categorised as the same histological type and grade, the T/N ratio was significantly different according to the presence or absence of this genetic alteration. Generally, 1p/19q deletion is found in 60–90% of OT,3 and the presence of these deletions is correlated with good chemosensitivity and longer survival, especially in grade III tumours.10 Although it is reported that 1p/19q deletion is exclusively associated with p53 overexpression or unmethylated MGMT,8 ,9 few biological features are linked to this chromosomal aberration. The lower rate of IDH1 mutation in anaplastic OT without 1p/19q deletion indicates that the high T/N ratio may reflect some aggressive biological features associated with unknown genetic or epigenetic changes similar to glioblastoma. The higher rate of contrast enhancement on MRI in the tumours without 1p/19q deletion in both grades, as shown in this study and in a previous report,18 may be associated with the higher T/N ratio. Contrast enhancement, which does not always correspond with methionine uptake, is regarded as labelling of metabolically active areas.18 ,19 In addition, grade II OT with 1p/19q deletion had T/N ratios within a narrow range around 2.0. This level is significantly lower than that in grade II tumours without the deletion, which had a wider range of the T/N ratio. This preoperative information is important because the operative procedures should be designed to avoid excessive resection of normal brain tissues, especially in OT with 1p/19q deletion, which are generally chemosensitive and radiosensitive and have good prognoses.
The uptake of amino acid into the cytoplasm is mainly dependent on a sodium-dependent transport system in the cell membrane, which is a regulator of cell growth and excess in tumour cells.20 ,21 The activity of the transport system is influenced by various factors including cell density, cellular proliferation rate, pH, hormones, growth factors and amino acid availability.14 ,15 ,21–23 Our previous study showed that the Ki-67 labelling index was correlated with the T/N ratio, especially in astrocytic tumours.17 Our present result showed that the 1p/19q status did not significantly associate with the Ki-67 labelling index or tumour cell density. These results indicate that the greater T/N ratio in OT without 1p/19q deletion compared with those with 1p/19q deletion does not simply reflect high proliferative activity or high cell density of the tumours.
Various imaging modalities have also been used to predict the 1p/19q status in OT. Jenkinson et al24 showed with MRI that an indistinct tumour border is more common in tumours with 1p/19q deletion than in those without the deletion. Other characteristic MRI features of 1p/19q deletion include heterogeneous signal intensity, diffuse and patchy enhancement, and frontal location.23–27 The apparent diffusion coefficient in diffusion-weighted images is negatively correlated with tumour cellularity and has no clear relationship with the 1p/19q status.27 ,28 The relative cerebral blood volume on perfusion-weighted images is correlated with 1p/19q deletion, but this observation has not reached universal agreement.28 ,29 PET has rarely been used to predict the 1p/19q status in gliomas.30 ,31 Walker et al31 showed that OT with 1p/19q deletion are more likely to have an increased metabolic state with either 18F-FDG PET or 201Tl single photon emission CT than those without the deletion. Using 11C-methionine PET, Saito et al32 reported a controversial result in which the T/N ratio of OT with 1p/19q deletion was significantly higher than the tumours without 1p/19q deletion. Although the relationship between the 1p/19q deletion and the T/N ratio in 11C-methionine PET should be investigated further in a larger cohort, we can predict that, when restricted to OT, the tumours without 1p/19q deletion are less likely to have IDH1 mutation and are more metabolically active than those with the deletions. Such more malignant features may be associated with higher 11C-methionine uptake in OT without the 1p/19 deletion. We should accumulate reliable research results to improve the accuracy of preoperative diagnosis of gliomas including their genetic status.
11C-methionine PET has been useful, to guide stereotactic biopsies, to delineate the target area for radiotherapy, to evaluate the response to therapy, and to differentiate between tumours and non-tumour lesions.33–35 Our previous study showed that the T/N ratio is significantly higher in grade II OT than in diffuse astrocytomas independent of the proliferative activity.17 The present result showed that the mean T/N ratio in grade III OT was significantly higher than that in grade II tumours, an observation that could not be verified in our previous study partly because of the insufficient sample number. Another important clinical application of 11C-methionine PET is proposed here, that is a preoperative prediction of the 1p/19q status of OT suspected by other imaging modalities.
The limitations of this study are the retrospective nature of the study design and the relatively small sample size. The important information about the treatment of gliomas obtained in this study using 11C-methionine PET needs to be validated in a larger prospective study.
References
Footnotes
YI and NSh contributed equally to this manuscript.
Contributors YI was involved in the design, data acquisition, analysis, conception and interpretation of the work, as well as drafting and revision of the manuscript. NSh was involved in data acquisition and analysis. TM was involved in monitoring data acquisition and supervised analysis. YU was involved in data acquisition and supervised analysis. NSa was involved in the conception and design of the manuscript. All authors have agreed with the final version of the manuscript and are accountable for all aspects of the work.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Chiba University Ethics Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.