Article Text

Abstract
Objectives To conduct an updated systematic review and meta-analysis of association between sleep and all-cause cognitive disorders.
Methods PubMed and EMBASE were searched from inception to 18 February 2019. Cohort studies exploring longitudinal associations of sleep with cognitive decline or dementia were included. The multivariable-adjusted effect estimates were pooled by random-effects models, with credibility assessment. The robust error meta-regression model was used to conduct the dose–response meta-analysis for sleep duration.
Results 11 155 reports were searched and 51 eligible cohorts with 15 sleep problems were included for our meta-analyses. Ten types of sleep conditions or parameters, including six (insomnia, fragmentation, daytime dysfunction, prolonged latency, rapid eye movement sleep behaviour disorder and excessive time in bed) with moderate-to-high levels of evidence, were linked to higher risk of all-cause cognitive disorders. Furthermore, a U-shaped relationship was revealed for the associations with sleep duration.
Conclusions Sleep management might serve as a promising target for dementia prevention.
- Sleep
- Dementia
- Cognitive decline
- Systematic review
- Meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Lines of evidence showed that sleep disorders could contribute to cognitive decline or dementia (cognitive disorders) and might serve as a promising target for dementia prevention. Evidence suggested sleep could influence core biomarkers of Alzheimer’s disease (AD). Difficulty in falling asleep,1 poor sleep quality,2 sleep loss,3 excessive daytime sleepiness4 and sleep disordered breathing5 were suggested to increase cerebral Aβ deposition in non-demented elderly. Apnoea6 or obstructive sleep apnoea syndrome7 was related to higher levels of AD-related neuronal injury biomarkers (ie, P-Tau and T-Tau). Sleep quality could even modulate the protective effects of other environmental factors such as physical exercise8 on brain Aβ deposition. Furthermore, prospective cohort studies have found that various sleep conditions or parameters, such as insomnia,9 obstructive sleep apnoea,10 sleep-related behaviours disorder,11 and changed sleep duration,12 could significantly elevate the risk of cognitive disorders among non-demented adults. However, the robustness of the evidence base might be jeopardised by sources of bias,13 such as high heterogeneity (due to for example, population characteristics, varying definitions of outcome and sleep-related exposures), recall bias and small-sample effect. In the past 2 years, large amounts of cohort studies have sprung up to explore the longitudinal influences of sleep-related exposures on incident risks of cognitive disorders, which necessitates an updated systematic review and meta-analysis.
Herein, we meta-analysed the associations between sleep (including insomnia and its components, sleep-related problems, sleep duration and change of sleep pattern) and all-cause cognitive disorders based on longitudinal cohort studies. Evidence ratings were performed according to risk of bias, inconsistency and imprecision.
Methods
Search strategy and selection criteria
We followed the recommendations by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 guidelines.14 15 PubMed and EMBASE were searched using the strategy: (((((((dementia) OR Alzheimer) OR cognition) OR cognitive)) AND ((((((((sleep) OR insomnia) OR sleepiness) OR somnolence) OR snoring) OR restless legs syndrome) OR periodic limb movement disorders) OR parasomnias))) AND risk, till 18 February 2019. Bibliographies of relevant original studies and systematic reviews were hand-searched in case of omission. The inclusion criteria were as follows: (i) the study used a longitudinal design that requires at least two measurements of cognition during follow-up, (ii) the study explored the association of sleep conditions or parameters with risk of dementia or cognitive decline and (iii) the study provided the risk estimates or the raw data that can be used to calculate these numbers. No restriction was applied on language. Studies were excluded if they met any of the following criteria: (1) risk estimate is not accessible, (2) cross-sectional studies, (3) only abstracts were available and (4) editorials or comments. Literature selection was performed by two experienced investigators (WX and C-CT) and any disagreements on inclusion were resolved by consensus and arbitration within the review team (WX, C-CT and LT).
Data extraction
Predesigned templates were used to extract the data, including first author, publication year, study design, cohort name, country, cognitive status at baseline, follow-up duration, attrition rate during follow-up, total sample size and incident case number for analysis, mean age, female percentage, outcome definition, type and measurement of sleep disturbance, adjusted confounders and the multivariable-adjusted risk estimates. If any data mentioned above were unavailable, we attempted to obtain them via contacting the corresponding authors. The data extraction was performed by two experienced investigators (WX and C-CT) and any discrepancies were addressed by negotiation with the third reviewer (LT).
Assessment of the study quality and credibility of meta-analyses
An evolving Newcastle-Ottawa Quality Assessment Scale (NOS) for observational cohort studies was employed to evaluate the quality of eligible studies. The total score of NOS was regarded here as a proxy to assess the overall risk of bias for each single study. The score for each item evaluated the associated risk of bias (online supplementary appendix 1). The credibility of each meta-analysis result was then categorised into four levels: ‘Good (G level)’, ‘Acceptable (A+/-level)’, ‘Susceptible (S+/-level)’ and ‘Poor (P level)’ according to a combined score of three domains: risk of bias, inconsistency and imprecision (online supplementary appendix 2). In particular, G and A+levels were regarded as moderate-to-high credibility. Publication bias was detected but not considered in evidence rating, because (1) not all meta-analyses were suitable for test of publication bias (number of included studies (N)<10) and (2) for those eligible, we found no evidence of publication bias (see the Results section).
Supplemental material
Statistical analyses
The multivariable-adjusted risk estimates and 95% CI were log-transformed and pooled using random models (DerSimonian-Laird method).16 Some studies reported odd ratios (ORs) but not relative risks (RRs) or HRs. Given that ORs tend to overestimate the effect sizes compared with RRs/HRs particularly when the incidence is not low, we transformed ORs to RRs using the following algorithm:17

P0 indicates the incidence of endpoint (dementia or cognitive decline) in the non-exposed group of cohort. When P0 is not available, the incidence rate of total sample was used as a proxy.17 A 95% prediction interval was calculated to better evaluate the precision of the result.18 Heterogeneity was assessed by Q test and quantified by the I2 metric . The source of heterogeneity was explored via sensitivity analyses, metaregression (if n≥10) and subgroup analyses according to multiple variables, including study design, region, gender, sample size, cognitive status at baseline, age stage (midlife vs late-life), follow-up duration, adjusted confounder (hypnotics, APOE4 and depression), outcome, exposure definition, effect estimate and quality score. The robustness of the results was examined by excluding those rated as at a higher risk of bias. Publication bias was assessed (if n≥10) following two steps: (1) testing the symmetry of the funnel plot by Egger method and (2) determining whether any asymmetry was due to publication bias via enhanced-contour funnel plots after the trim-and-fill method.
Taking into account the following cases wherein results might be biassed, multiple subgroup and sensitivity analyses were conducted. First, some studies recruited people without dementia at baseline and others specifically constrained the population to those with unimpaired cognition. Notably, inclusion of individuals with mild cognitive impairment, who might be at prodromal stage of AD, resulted in a degree of misclassification bias, especially when the population was in their advanced age and was followed insufficiently. Thus, subgroup analyses according to the cognitive status at baseline, follow-up sufficiency (Q7 of NOS) and life-stage were performed. Moreover, sensitivity analyses excluding studies with poor generalisability (Q1), inadequate follow-up (Q7) and high attrition rates (Q8) were conducted (Appendix 1). The ‘metagen’, ‘metabias’ and ‘trimfill’ packages in R V.3.4.3 software (https://www.r-project.org) were used to perform all these analyses.
A U-shape relationship was indicated for the association between dementia and sleep duration. In the present study, we first summarised the risk estimates based on the comparison of the extreme categories (highest vs middle level and lowest vs middle level). Separate analyses according to outcome (dementia or cognitive decline, AD and VD) and exposure (nocturnal and total daily duration including daytime naps) were performed. Next, we examined the exposure–response relationship between sleep duration and cognitive disorders for non-linearity by fitting a restricted cubic spline model. We used the inverse variance weighted least squares regression with cluster robust error variances (REMR model).19 20 For studies wherein the reference group was not the lowest category (eg, exposure was defined as tertiles and the middle one is set as the reference group), we regraded the lowest category as the reference and recalculate the effect size using the method by Orsini.21 We assigned the midpoint of the upper and lower boundaries in each category of sleep duration as the average level. For studies with an open-ended boundary; we multiplied or divided the reported boundary by 1.25. Stata V.12.0 was used to conduct the dose–response analyses.
Results
Searching results
Figure 1A exhibits the flow diagrams of the study selection process. The search yielded 11 155 articles after deduplication. After scanning the titles and abstracts, 72 articles were considered as potentially eligible. After reviewing the full-texts, we further excluded 16 literatures for varied reasons (figure 1A). After further integrating with additional four papers from the bibliography, a total of 51 cohorts in North America (43%), Europe (37%) and East Asia (20%) were finally included (online supplementary appendix 3).

Search flowchart and summary characteristics of included studies. The search yielded 11 155 literatures after deduplication. After the standardised literature selection, a total of 51 literatures on 41 cohorts in North America (43%), Europe (37%) and East Asia (20%) were finally included (A). Most studies reported the association of sleep problems with dementia (61%), AD (39%) or cognitive decline (41%) and only a few involved VD (16%) (B). In these studies, we found eight types of sleep-related problems and seven insomnia-related characteristics for meta-analyses (C). AD, Alzheimer’s disease; OR, odds ratio; RR, relative risk; TIB, time in bed.
Characteristics of studies
The detailed characteristics of studies included in the meta-analysis are shown in table 1. Most studies reported the association of sleep with dementia (61%), AD (39%) or cognitive decline (41%) and only a few involved VD (16%) (figure 1B). In these studies, we found 15 types of sleep-related exposures eligible for meta-analyses, including insomnia, inadequate/overlong sleep duration, sleep behavioural disturbance (SBD), apnoea, long time in bed (TIB), snoring, napping, and change in sleep pattern and seven insomnia components (including daytime dysfunction, efficiency, fragmentation, adequacy, frequency, latency and subjective quality) (figure 1C).
Characteristics of 51 studies included in the meta-analysis
Insomnia and cognitive disorders
Insomnia was significantly associated with 27% higher risk of cognitive disorders (RR=1.27, 95% CI=1.16 to 1.39, I2=82%) after pooling findings of 23 cohort studies (260 915 participants and 30 027 incident cases). Meta-regression revealed that no factors can explain the source of heterogeneity. Sensitivity analysis excluding three studies22–24 will lower I2<40% without influence on the significance of the primary result (RR changed from 1.27% to 1.19. 95% CI=1.12 to 1.25). Subgroup analysis indicated that the significance of the primary result was not altered by study design, region, gender, cognitive status at baseline, age stage, effect estimate, quality score or AD as an outcome (figure 2). However, the pooled results tend to be non-significant in strata of small-sample studies, studies with longer follow-up, studies adjusting for more covariates, studies with VD as outcome and insomnia defined as continuous variable (figure 2). The conclusions seemed more homogeneous in middle-aged population than late-life elderly. No publication bias was revealed for primary (p=0.183) or subgroup analyses.

Association of insomnia with risk of cognitive disorders. Subgroup analyses indicated that the significance of the primary result was not altered by study design, region, gender, cognitive status at baseline, age stage, effect estimate, quality score or AD as an outcome. However, the pooled results tend to be non-significant in strata of small-sample studies, studies with longer follow-up, studies adjusted for more covariates, studies with VD as an outcome or insomnia defined as a continuous variable. AD, Alzheimer’s disease; MCI, mild cognitive impairment; RR, relative risk.
Components of sleep disorder and cognitive disorders
The high heterogeneity observed above might be explained by heterogeneous definitions of sleep disorder (online supplementary appendix 3). To validate this hypothesis, we conducted separate meta-analyses according to different components. Among seven components for meta-analyses, four were associated with 7%–16% increased risk of cognitive disorders, including daytime dysfunction (RR=1.16, 95% CI=1.06 to 1.27, I2=38%), inefficiency (RR=1.15, 95% CI=1.02 to 1.30, I2=83%), fragmentation (RR=1.11, 95% CI=1.05 to 1.17, I2=0%) and latency (RR=1.07, 95% CI=1.00 to 1.15, I2=26%). Adequacy, high frequency of insomnia, and subjective quality showed no significant associations in primary analyses (figure 3).

Associations between components of insomnia and cognitive disorders. Four insomnia components were associated with 7%–16% increased risk of cognitive disorders, including daytime dysfunction, inefficiency, fragmentation and latency. Adequacy, high frequency of insomnia and subjective quality showed no significant associations in primary analyses. RR,relative risk.
Despite low heterogeneity, meta-regression revealed that sample size (p<0.05 for latency) and exposure definition (p<0.005 for daytime dysfunction) could fully explain the source of heterogeneity. In subgroup analyses, inadequacy was associated with 25% higher risk of dementia (RR=1.25, 95% CI=1.04 to 1.44, I2=18%) and inefficiency could elevate the risk of cognitive decline by 24% (95% CI=1.03 to 1.50, I2=31%) when it was defined categorically (online supplementary appendix 4).
Sleep-related problems and cognitive disorders
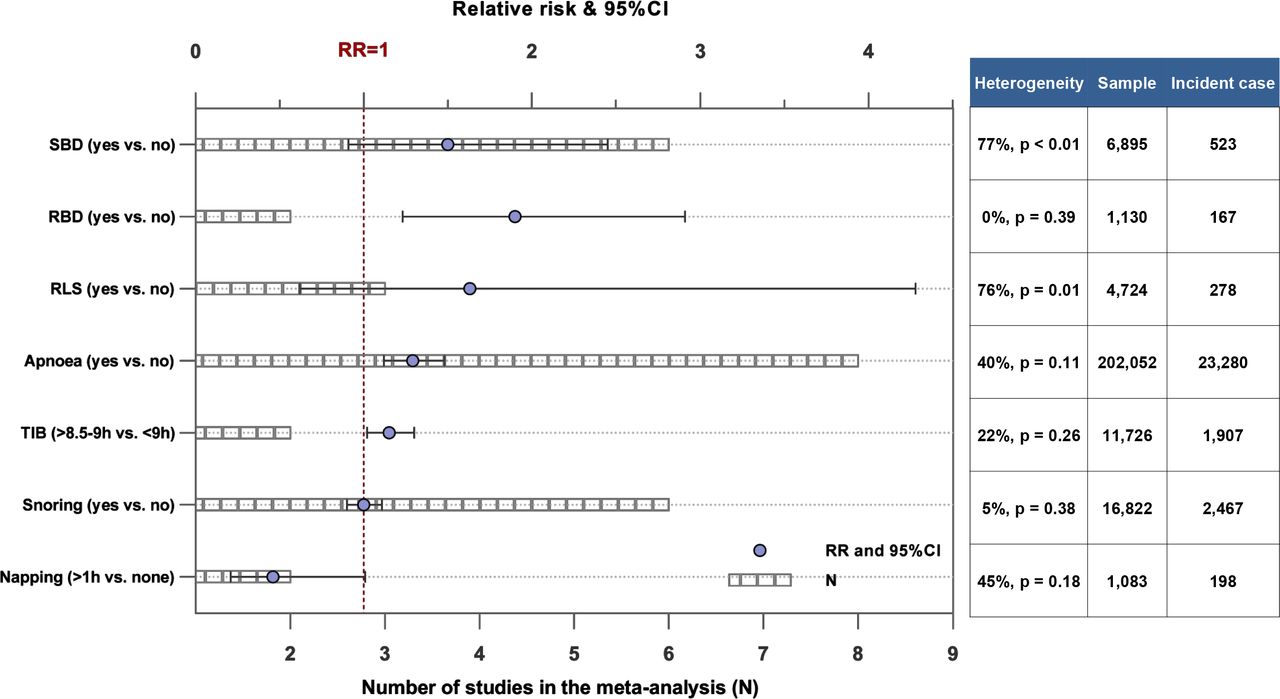
We also identified four other types of sleep-related problems that showed significant associations with risk of cognitive disorders, including rapid eye movement sleep behavioural disorder (RBD, RR=1.90, 95% CI=1.23 to 2.91, I2=0%), apnoea (RR=1.29, 95% CI=1.12 to 1.48, I2=40%), long TIB (RR=1.15, 95% CI=1.02 to 1.30, I2=22%) and habitual napping (high trend: RR=0.46, 95% CI=0.21 to 1.01, I2=45%). We identified no significant association with restless leg syndrome (RLS) or snoring (figure 4). Subgroup or sensitivity analyses did not change the above results.
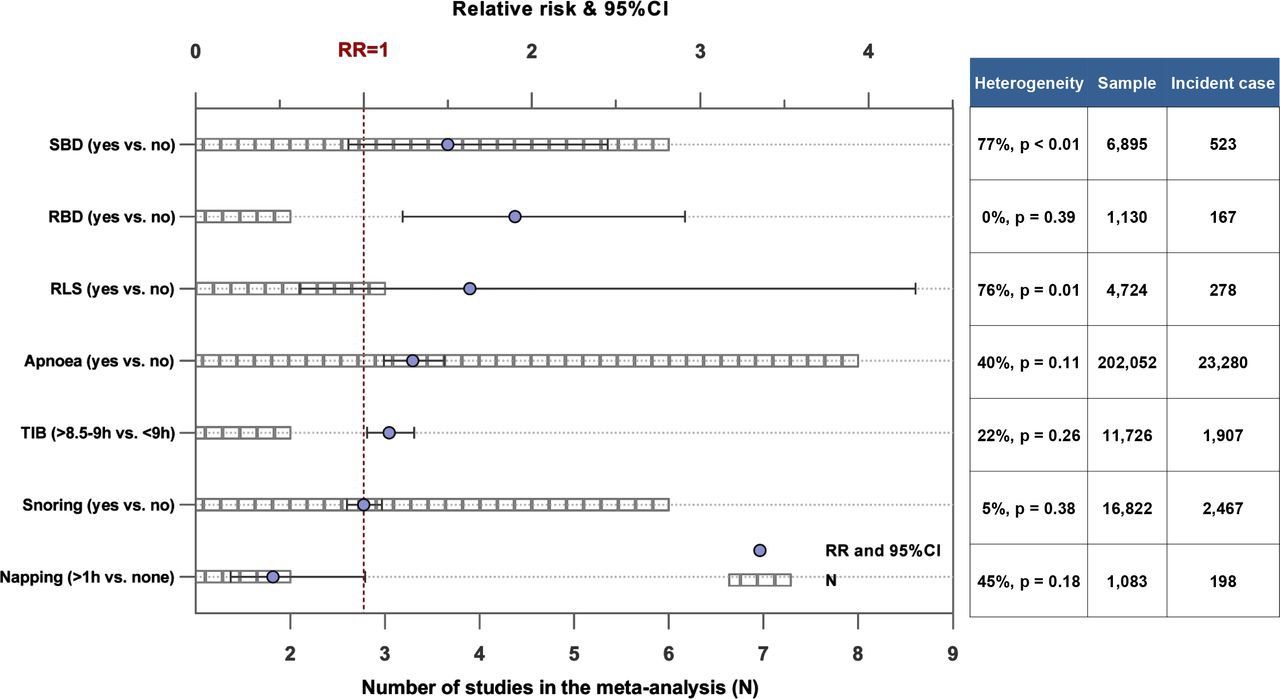
Associations of sleep-related problems with cognitive disorders. Four types of sleep-related problems showed significant associations with risk of cognitive disorders, including rapid eye movement sleep behavioural disorder (RBD), apnoea, longer time in bed (TIB) and habitual napping. We identified no significant association with restless leg syndrome (RLS) or snoring. RR, relative risk; SBD, sleep behavioural disturbance.
Sleep duration and cognitive disorders
A total of 21 prospective cohort studies reported the association between sleep duration and cognitive disorders. Three studies25–27 that used continuous variables and one repetitive sample28 were excluded, leaving 17 for meta-analyses (including 12 for nocturnal and five for total daily duration). All studies are prospective cohort studies with populations from North America (two in Canada and seven in America), Europe (one in Finland, one in Spain and two in Sweden) and East Asia (one in China, one in South Korea and two in Japan). The mean age varied from 51 to 83 years old and the mean follow-up varied from 1 to 22.6 years. The average study quality is moderate (median score=7).
A nonlinear trend was revealed for the relationship between sleep duration and cognitive disorders. Subgroup analyses indicated that the trend persists for AD, but not for VD (table 2). The dose–response analyses revealed significant nonlinear associations between sleep duration and risks of cognitive disorders (p=0.0003 for nocturnal and p=0.017 for total daily duration) or AD (p=0.018 for nocturnal) (figure 5). Specifically, as for the sleep duration at night, the optimal duration was found to be roughly 5.6–6 hours for lower risk of cognitive disorder (figure 5A) and 5.6–7 hours for lower risk of AD (figure 5B). The risk of cognitive disorder (figure 5A) or AD (figure 5B) will be significantly elevated when the nocturnal sleep duration is over 10 hours or less than 4 hours. Similar results were obtained for the associations with total daily sleep duration: the protective window was situated between 5.6 and 9 hours for lower risk of cognitive disorders (figure 5C). The nonlinearity in the relationship between daily duration and AD (figure 5D) or VD showed borderline significance (p=0.069), possibly because of the limited number of included studies.
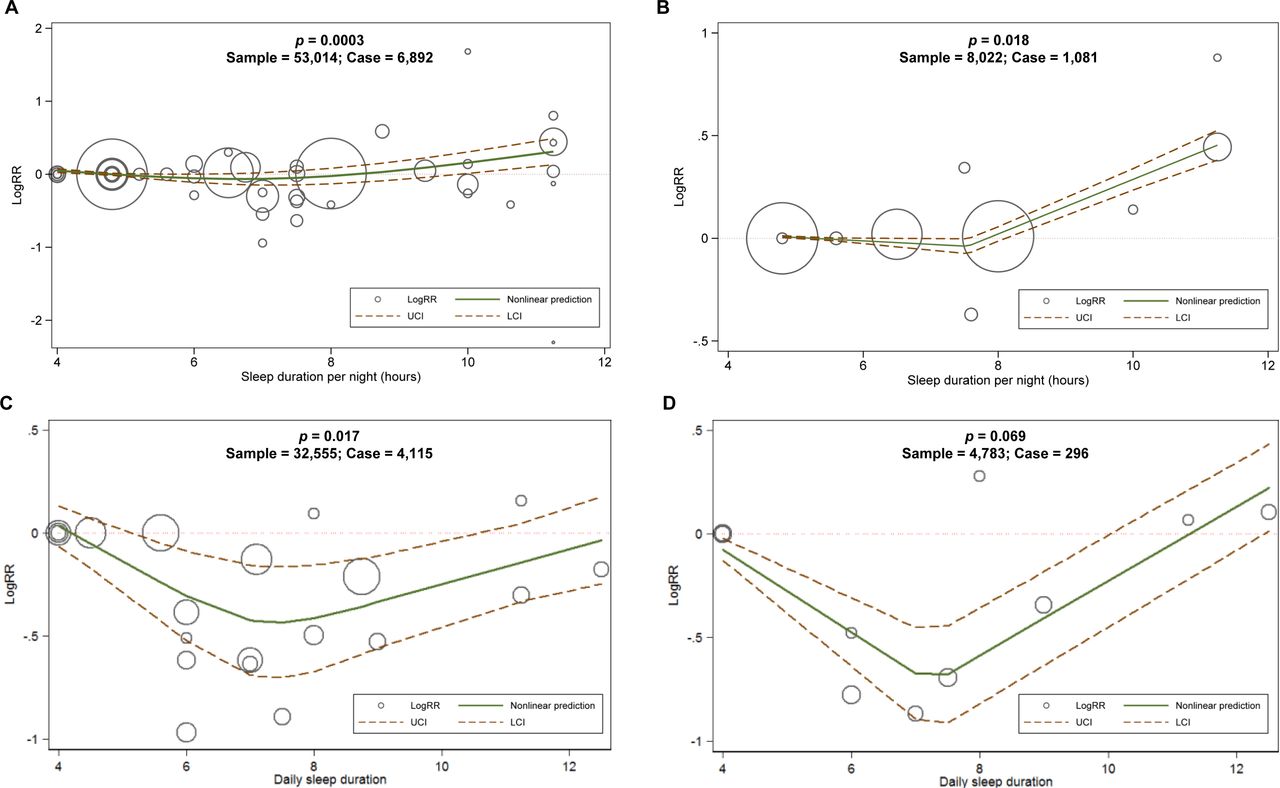
Dose–response relationships between sleep duration and cognitive disorders or AD. The dose–response analyses revealed significantly nonlinear associations between nocturnal or total daily sleep duration and risk of cognitive disorders (A and C) or AD (B and D). AD, Alzheimer’s disease; RR, relative risk.
Qualitative syntheses for the relationship between sleep duration and cognitive disorders
Change of sleep characteristics and cognitive disorders
Moreover, several studies reported associations between cognitive decline and change of sleep pattern,29 that is, change in sleep characteristics, including duration,12 30–32 depth,32 latency30 and variability.33 Meta-analyses of change in sleep duration found that increased duration rather than reduced duration could significantly elevate the risk of cognitive disorders in non-demented elderly (online supplementary appendix 5).
Rating of evidence levels
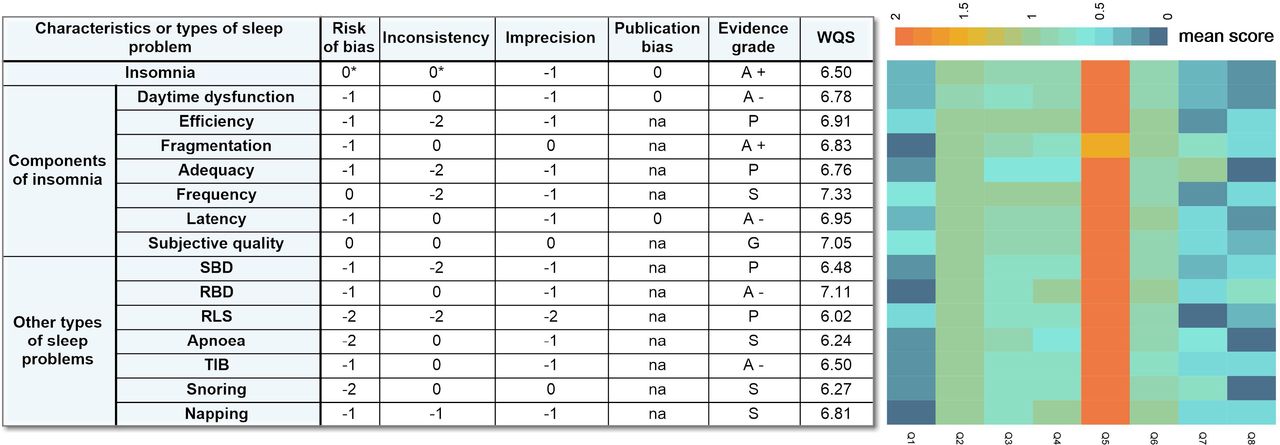
As for the levels of credibility, three meta-analyses (insomnia, fragmentation and subjective quality) were rated at a moderate-to-high level (G and A+level) and four (daytime dysfunction, latency, RBD and TIB) were rated at a moderate level (A- level). In addition, we found that eight meta-analyses were rated at S level (frequency, apnoea, snoring and napping) or P level (efficiency, adequacy, SBD and RLS). Poor generalisability, follow-up inadequacy and attrition are major sources of bias (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Evidence rating for meta-analyses results. Three meta-analyses (insomnia, fragmentation and subjective quality) were rated at a moderate-to-high level and four (daytime dysfunction, latency, RBD and TIB) were rated at a moderate level. In addition, we found that eight meta-analyses were rated at S level or P level. Poor generalisability, follow-up inadequacy and large attrition are major sources of bias. RBD, rapid eye movement sleep behavioural disorder; RLS, restless leg syndrome; SBD, sleep behavioural disturbance; TIB, time in bed.
Discussion
We found evidence supporting 10 types of self-reported sleep conditions or parameters, including six (insomnia, fragmentation, daytime dysfunction, prolonged latency, RBD and excessive TIB) with moderate-to-high levels of evidence and four (apnoea, no habitual napping, inefficiency, increased sleep duration) with low levels of evidence, as predictors of higher risk of cognitive disorders in non-demented adults. The quantitative meta-analysis indicated that either insufficient (<4 hours per night or total daily) or excessive (>10 hours per night and >12.5 hours for total daily) sleep duration could elevate risk of all-cause cognitive disorders or AD dementia.
The high heterogeneity observed for association between insomnia and cognitive disorders might be explained by the varying definitions of insomnia. The heterogeneity levels were significantly lowered when the analyses were restricted to its component domains (such as daytime dysfunction, fragmentation, latency and subjective quality). As for the subtypes of cognitive disorders, insomnia tends to influence risk of AD but not VD. However, the associations between AD and insomnia components have been scarcely reported34 and should be further investigated in the future (online supplementary appendix 4). Interestingly, the associations became non-significant when specific factors (hypnotics, APOE4 status and depression at baseline) were included as covariates, suggesting the potential existence of stratified or mediating effects. The mechanisms underpinning the association with insomnia might be related to inflammation.35
We found that apnoea is another important sleep-related risk factor for all-cause cognitive disorders. Obstructive sleep apnoea has been previously linked with poorer performance in multiple cognitive domains among non-demented individuals, including attention, executive functioning, visuospatial and constructional abilities and psychomotor speed.36 The mechanism might be related to long-term cerebral hypoxia and hypometabolism, which might contribute to loss of regional cortex and white matter hyperintensities in the hippocampus and cingulate cortex.35
A U-shaped relationship was confirmed between self-reported nocturnal or total daily sleep duration and all-cause cognitive disorders or AD, which is consistent with previous findings.37 One meta-analysis37 incorporating five cohorts and four cross-sectional studies suggested the optimal sleep duration approximate 7 hours, which is slightly different from ours (6.3 hours at night and 7.3 hours for total daily sleep duration). Because we included 17 cohort studies for dose–response analyses and conducted separate analyses for the nocturnal and total daily sleep durations. The underlying mechanisms might be explained by that shorter or longer sleep duration contributes to faster atrophy in frontotemporal region,38 ventricular enlargement39 and hippocampal degeneration.40 Another possible explanation is that those who already have somedegeneration, or other comorbidities and medication use tend to sleep longer.
Compared with previous meta-analyses (online supplemenatry appendix 6), the present study had several significant advantages: (1) only longitudinal cohort studies were included, (2) the sleep disorder spectrum was fully covered and separately explored for each domain, (3) as an updated systematic review, we included 33 other literatures compared with the latest systematic review,13 (4) the dose–response relationship for sleep duration was explored, (5) stratified analyses according to different types of sleep or cognitive disorders were conducted to lower the heterogeneity of the pooled results and (6) evidence robustness was rated.
Several limitations exist. First, the associations identified by the analyses based on observational cohort studies were not equal to causal relationships. Randomised controlled trials are warranted in the future to test the roles of sleep management in preventing cognitive decline or dementia. Second, we did not explore the association of hypnotics with risk of cognitive disorders in the present study though they were closely linked with sleep. Instead, we conducted subgroup analyses according to whether sleep medication was included as a covariate. Third, the associations with dementia subtype (AD or VD) were not thoroughly investigated due to the limited evidence. Fourth, the influences of important confounders, such as cardiovascular diseases are not fully explored,
In conclusion, the findings of the our study provided varying levels of evidence that 10 types of sleep-related exposures were linked to increased risk of all-cause cognitive decline or dementia. Future studies are warranted to confirm the associations with AD and to examine the roles of sleep management in benefiting cognition and lowering risk of dementia.
References
Footnotes
Twitter @na
Contributors WX: conceptualisation and design of the study, collection and analysis of the data, drafting and revision of the manuscript, and prepared all the figures. C-CT: collection and analysis of the data, and revision of the manuscript. J-JZ, X-PC and LT: revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.