Article Text

Abstract
Chronic hypoxaemia in chronic obstructive pulmonary disease is a well known risk factor for polyneuropathy but the impact of intermittent hypoxaemia on peripheral nerve function has not been established so far. A case-control study was performed to evaluate the prevalence of polyneuropathy in obstructive sleep apnoea (OSA). Out of 24 patients with OSA, 17 (71%) had clinical signs of polyneuropathy versus seven (33%) out of 21 matched controls. The mean amplitude of the sural sensory nerve action potential was smaller in the OSA group than in the control group, indicating axonal nerve damage. The differences were significant and could not be attributed to other known risk factors for polyneuropathy. The severity of axonal damage in patients with OSA correlated with the percentage of the night time with an O2saturation below 90%. It is assumed that recurrent intermittent hypoxaemia in OSA is an independent risk factor for axonal damage of peripheral nerves.
- polyneuropathy
- obstructive sleep apnoea
- hypoxaemia
Statistics from Altmetric.com
Patients with obstructive sleep apnoea (OSA) experience numerous repetitive apnoeic events during sleep caused by partial or complete upper airway occlusions. The results are intermittent hypoxia and hypercapnia. In the CNS neuropsychological impairment, including excessive daytime sleepiness and an increased risk for stroke, are features of the disease.1-3
There are several studies indicating an increased prevalence of polyneuropathy in chronic obstructive pulmonary disease (COPD).4-7 In a large multicentre study investigating 151 patients with COPD, the rate and the severity of the polyneuropathy correlated with the severity of the chronic hypoxaemia.6
We conducted a case-control study to determine the occurrence of polyneuropathy in OSA and to investigate whether intermittent hypoxia has to be regarded as a risk factor for polyneuropathy. Subjects with other known risk factors for polyneuropathy were excluded from the study and groups were exactly matched for possible independent variables such as age, body mass index (BMI, weight/(height)2) and alcohol intake. This was crucial as patients with OSA are known to be prone to several known risk factors for polyneuropathy.8
Patients and methods
PATIENTS
Twenty four patients with newly diagnosed OSA were included into the study. The disease was diagnosed when the apnoea+hypopnoea index (AHI; number of episodes of apnoea+hypopnoea/hour of sleep) was 10 or greater. The 21 controls had no clinical signs or symptoms of OSA and were admitted to hospital for transient ischaemic attack (n=6), depression (n=10), pseudotumour cerebri (n=3), and transient global amnesia (n=2). To exclude oligosymptomatic OSA, polysomnography was performed in all 21 controls, and only subjects with an AHI of 5 or less were accepted as controls. Patients with OSA and controls with a known cause of polyneuropathy such as diabetes mellitus, renal failure, carcinoma, alcoholism, disorders of immune mediated injury, and use of neurotoxic drugs were excluded from the study. The mean alcohol intake/week was asked for.
CLINICAL EXAMINATION
Probable polyneuropathy was diagnosed clinically when at least two of the following three clinical signs were found: (1) peripheral motor weakness; (2) sensory loss (at least reduction of pallaesthesia⩽5/8); (3) hyporeflexia or areflexia. Possible polyneuropathy was diagnosed when one clinical sign was found.
POLYSOMNOGRAPHY
Overnight polysomnography was performed in a standard manner (Brainlab, Schwarzer, Germany) and scored manually according to the criteria of Rechtschaffen and Kales.9 Mean and minimal arterial O2 saturation (mean and minimum SaO2) by fingertip oximetry, AHI, and percentage of night time with an O2 saturation below 90% (CT90) were recorded.
NEUROGRAPHY
Nerve conduction studies were performed on a Keypoint electroneurographical system (Dantec, Denmark) using standard techniques as described elsewhere.10 The base to peak amplitude of the sensory nerve action potential (SNAP) of the left sural nerve, the sensory conduction velocity (CV) of the left sural nerve, the base to peak amplitude of the compound muscle action potential (CMAP) of the right extensor digitorum brevis muscle after stimulation of the peroneal nerve at the ankle, and the motor CV of the right peroneal nerve were determined.
STATISTICAL ANALYSIS
Results are expressed as mean (SD), and were analysed with non-parametric tests. The Mann-Whitney Utest was used to compare unpaired data (population characteristics, BMI, alcohol intake, and laboratory data). The difference in the prevalence of polyneuropathy was calculated with Yates' corrected χ2 test. Regression analyses were performed to assess correlations between the amplitudes of the SNAPs and different polysomnographical variables and age. The level of significance was set at p⩽0.05.
Results
The OSA and control group were well matched for sex, age, BMI, and alcohol intake.
Haemoglobin A1C, creatinine, and hepatic enzyme concentrations were within the normal laboratory range in all subjects, with no significant differences between the groups (table1).
Characteristics of patients with OSA and controls. Prevalence of PNP and electrophysiological data in patients with OSA and controls
The AHI was 38.5 in patients with OSA versus 4.4 in controls (p<0.01), the mean SaO2 was 92.1% versus 94.5% (p<0.01), the minimum SaO2 was 77.3% versus 85.4% (p<0.01), and the CT90 was 25.8% versus 4.0% (p<0.01).
Neurological examination disclosed at least one clinical sign of polyneuropathy in 17 out of 24 patients with OSA (71%) and in seven out of 21 controls (33%, p<0.05). In the OSA group, 10 patients (42%) had at least two clinical signs of polyneuropathy and were diagnosed as probable clinical polyneuropathy, and seven patients with one sign were classified as possible polyneuropathy. In the control group, one subject (5%) had more than one clinical sign of polyneuropathy, and six had one.
In the OSA group, 10 of the 17 patients with clinical signs of polyneuropathy reported numbness of the toes or feet, three additionally dysaesthesia of the legs, three additionally a slight sensory ataxia, and two additionally dysaesthesia and ataxia. Seven patients with OSA with possible clinical polyneuropathy were asymptomatic. In the control group two of the seven patients with at least one clinical sign of polyneuropathy had noticed numbness of the toes, one numbness and a slight sensory ataxia. Four were asymptomatic.
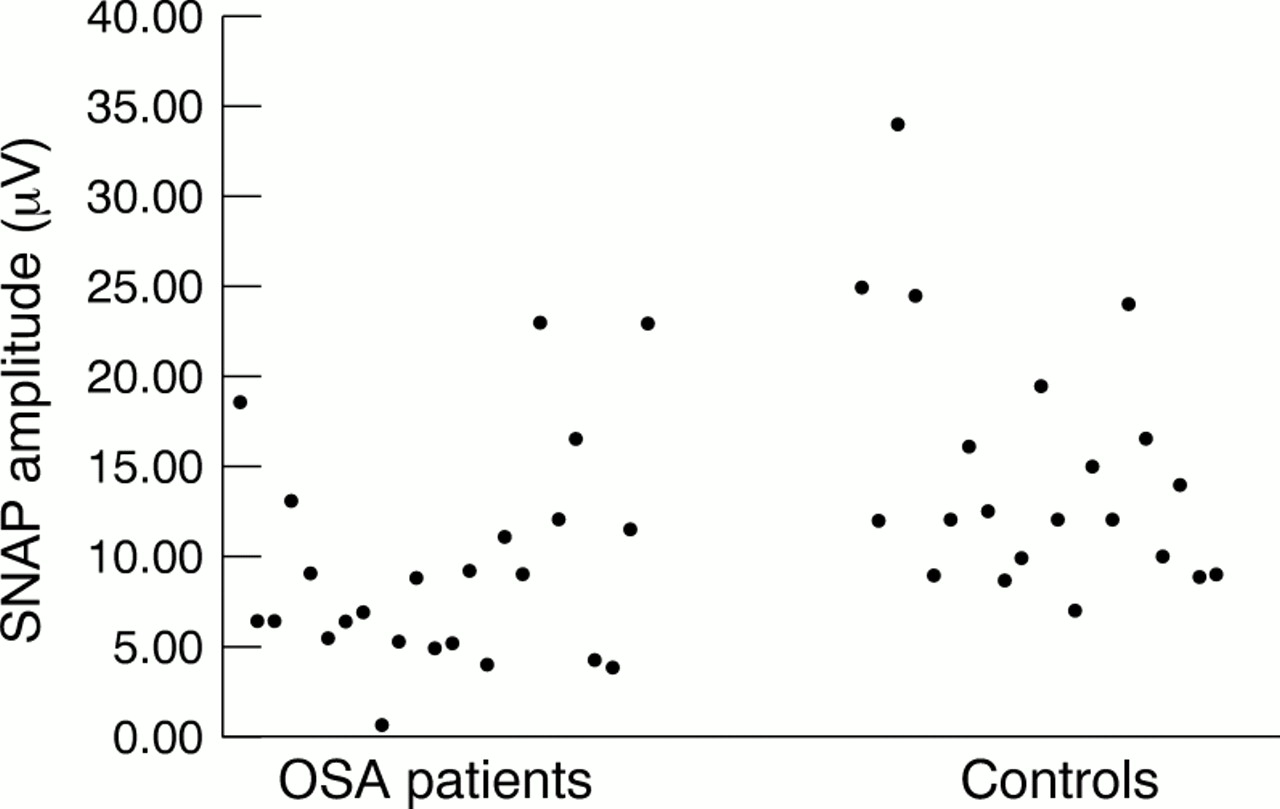
The differences in the prevalence of probable and possible clinical polyneuropathy were significant (p<0.05; Yates). The amplitudes of the SNAPs differed significantly, with smaller amplitudes in the OSA group than the control group (fig 1, table 1). Peroneal CMAPs and CVs did not differ between the groups (table1).
{kind=link}
Amplitudes of the SNAPs of the OSA group and the control group.
In the OSA group a significant negative correlation was found for the SNAPs and the CT90 (r=–0.43, p<0.05). No significant correlation was found for the SNAPs and the AHI, the mean SaO2, the minimum SaO2, or the age.
Discussion
Our data show an increased prevalence of polyneuropathy in patients with OSA. This cannot be attributed to other known risk factors of polyneuropathy. The reduced amplitude of the SNAPs in the OSA group indicates axonal nerve damage. The severity of axonal damage correlates with the CT90, which represents the duration of marked arterial hypoxaemia.
Our findings accord with a recent study which investigated 17 patients with very severe OSA (AHI⩾40 and minimum SaO2⩽80%) and 10 control patients neurographically.11 These authors found smaller amplitudes for sensory and mixed nerve action potentials in patients with OSA.
According to the clinical criteria, the prevalence of possible or probable polyneuropathy in our study was 71%. The severity was mild and no patient had severe disability due to polyneuropathy. The prevalence of polyneuropathy in OSA is similar to its prevalence in patients with chronic obstructive pulmonary disease (COPD), which varies between 28%6 and 80%.7 The numbers strongly depend on the diagnostic methods and criteria applied. In accordance with our findings, electrophysiology and nerve biopsy in COPD suggest axonal degeneration as the main pathophysiological feature of polyneuropathy with only a slighter degree of demyelinisation.12
A prevalence of 33% possible or probable clinical polyneuropathy in our control group seems to be unusually high but results from the fact that it was diagnosed regardless of whether the subjects had symptoms of polyneuropathy or not. A large field screening investigation demanding two symptoms additionally to clinical signs for the diagnosis of polyneuropathy found a prevalence of 10.9% in Italy.13Applying the Italian diagnostic criteria to our study population, the prevalence fell to 5% possible or probable symptomatic polyneuropathy in the control group, reflecting the fact that known reasons for polyneuropathy were excluded in our study.
In animal models, chronic hypoxaemia causes a deceleration in nerve conduction velocity.14 Studies of the oxygen consumption in the microenvironment of the peripheral nerve under conditions of nerve oedema15 and experimental diabetic neuropathy16 show that the peripheral nerve function is oxygen dependent. Nerve capillary endothelial cell hyperplasia occurs in hypoxic neuropathy and predisposes to endoluminal occlusion. Additionally, thickening of the nerve perineurium occurs and can impede transport of nutrients and oxygen.17 Axonal transport is an energy requiring process and its impairment by hypoxaemia can enhance or cause axonal degeneration.18 19 We conclude that nerve function critically depends on a sufficient oxygen supply.
Experimental chronic hypoxaemia causes a resistance to ischaemic conduction block (RICB), also seen in diabetic neuropathy.14 20 The RICB is likely to be an adaption to endoneurial hypoxaemia caused by reduced O2 requirements or a more efficient anaerobic metabolism. In hypoxaemia, the adaptive mechanism is delayed, as 4 weeks of exposure to normobaric 10% hypoxaemia are needed to induce RICB.14 Mayeret al 11 found RICB in seven out of 17 patients with OSA characterised by a low mean nocturnal arterial O2 saturation. They treated seven patients with OSA (four of them with RICB, three without) with nasal continuous positive airway pressure (CPAP) for 2 months. The RICB disappeared in the four patients, whereas axonal neuropathy remained unchanged in all seven patients. Whether or not polyneuropathy is reversible by prolonged continuous CPAP therapy has to be investigated by a longitudinal therapeutic intervention study.
We conclude that recurrent intermittent hypoxaemia is an independent risk factor for axonal damage of peripheral nerves.
Acknowledgments
The expert technical assistance of Angelika Okegwo is gratefully acknowledged.