Article Text

Abstract
OBJECTIVES To assess the frequency of hyperthermia in a population of acute neurosurgical patients; to assess the relation between brain temperature (ICT) and core temperature (Tc); to investigate the effect of changes in brain temperature on intracranial pressure (ICP).
METHODS The study involved 20 patients (10 severe head injury, eight subarachnoid haemorrhage, two neoplasms) with median Glasgow coma score (GCS) 6. ICP and ICT were monitored by an intraventricular catheter coupled with a thermistor. Internal Tc was measured in the pulmonary artery by a Swan-Ganz catheter.
RESULTS Mean ICT was 38.4 (SD 0.8) and mean Tc 38.1 (SD 0.8)°C; 73% of ICT and 57.5% of Tc measurements were ⩾38°C. The mean difference between ICT and Tc was 0.3 (SD 0.3)°C (range −0.7 to 2.3°C) (p=0. 0001). Only in 12% of patients was Tc higher than ICT. The main reason for the differences between ICT and Tc was body core temperature: the difference between ICT and Tc increased significantly with body core temperature and fell significantly when this was lowered. The mean gradient between ICT and Tc was 0.16 (SD 0.31)°C before febrile episodes (ICT being higher than Tc), and 0.41 (SD 0.38)°C at the febrile peak (p<0.05). When changes in temperature were considered, ICT had a profound influence on ICP. Increases in ICT were associated with a significant rise in ICP, from 14.9 (SD 7.9) to 22 (SD 10.4) mm Hg (p<0.05). As the fever ebbed there was a significant decrease in ICP, from 17.5 (SD 8.62) to 16 (SD 7.76) mm Hg (p=0.02).
CONCLUSIONS Fever is extremely frequent during acute cerebral damage and ICT is significantly higher than Tc. Moreover, Tc may underestimate ICT during the phases when temperature has the most impact on the intracranial system because of the close association between increases in ICT and ICP.
- head injury
- subarachnoid haemorrhage
- brain temperature
- intracranial pressure
Statistics from Altmetric.com
Cerebral temperature has been recognised as a strong factor in ischaemic brain damage. Laboratory investigations have shown that intraischaemic hypothermia may limit brain damage.1-4 The classic mechanism proposed for this protection is a lowering of oxygen and glucose consumption sufficient to permit tolerance to prolonged periods of oxygen deprivation. Hypothermia reduces the brain's energy requirements by slowing the activation metabolism required for neuronal function and the residual metabolism necessary to maintain neuronal activity.5
By contrast with hypothermia, brain hyperthermia worsens outcome in several animal models of brain injury. For example, in models of cerebral ischaemia intraischaemic hyperthermia led to more severe neuronal and cerebrovascular consequences.6 7 Even a delayed post-traumatic hyperthermia (4 days after a fluid percussion injury) led to significantly increased mortality, blood-brain barrier damage, and axonal damage.8 These experimental findings were partially confirmed in the clinical setting.
Many clinical studies have set out to assess the effectiveness of prophylactic and delayed moderate hypothermia for improving neurological outcome and controlling intracranial hypertension after head injury.9 10 Moderate hypothermia may improve outcome at 3 and 6 months in patients admitted with a Glasgow coma score (GCS) between 5 and 7.11 However, further studies failed to show that moderate hypothermia is a safe and effective treatment in brain damage.12 On the other hand an association was found between hyperthermia and initial stroke severity, infarct size, mortality, and outcome in 390 patients admitted with acute stroke.13 Even though it has not been proved whether this relation is causal or not, the highly significant difference in outcome between hypothermic, normothermic, and hyperthermic patients is surprising. In head injury too a strong association has been found between the duration of fever and poor outcome.14
In the clinical setting the impact of changes in temperature on the progression of ischaemic lesions is less clear cut than in the laboratory setting, but there is definitely a relation between ischaemic injury and temperature.13 14 This suggests that failure to control brain temperature during the acute phase might affect neurological recovery from brain damage. Maintenance of normothermia has, therefore, been included by many authors in the first line management of severe head injury.15
However, the efficacy of maintaining normothermia has not been assessed and these considerations are based on the assumption that core (or rectal) temperature reflects cerebral temperature. Moreover, many reports indicate that systemic temperature may be quite different from brain temperature and the pathophysiological basis of such differences are not fully understood.
This work was therefore designed with the following aims:
-
To assess the frequency of hyperthermia in a population of acute neurosurgical patients
-
To assess the relation between brain temperature (ICT) and core temperature (Tc)
-
To investigate the effect of changes in brain temperature on intracranial pressure (ICP).
Materials and methods
Brain temperature monitoring was approved by the ethics committee of our institution. The study involved 20 acute neurosurgical patients admitted to the Neurosciences intensive care unit of the Ospedale Maggiore Policlinico of Milan; 10 had severe head injuries (SHI), eight subarachnoid haemorrhages (SAHs), and two neoplasms.
CLINICAL MANAGEMENT AND MONITORING
Management of SHI was based on early evacuation of surgical masses and prevention and treatment of secondary insults. In seven of the eight patients with SAH a ruptured aneurysm was diagnosed and operated on. Surgical clipping was always done within 72 hours from the bleeding.
Mean arterial blood pressure (MAP) and ICP were managed to ensure a cerebral perfusion pressure (CPP) of at least 60 mm Hg in SHI and 70 mm Hg in SAH. An ICP>20 mm Hg during the first 3 days and >25 mm Hg after that were considered as thresholds for treatment. Treatment included sedation, CSF drainage, mild or moderate hyperventilation, and mannitol. In cases of refractory intracranial hypertension barbiturates or surgical decompression were considered.
In patients with SAH ventriculostomy was performed to treat acute hydrocephalus. In these patients CSF was drained for 50 minutes/hour and ICP was recorded for the remaining 10 minutes. In two patients with tumours the ventricular catheter was placed to control intracranial hypertension by CSF drainage.
In 15 patients the internal jugular bulb was cannulated, in 10 of them by a 4F catheter for intermittent determination of oxyhaemoglobin saturation in the jugular vein (SjO2). In five patients SjO2 was continuously monitored by a fibreoptic catheter (Abbott Oximetric). The correct position of the tip of the catheters was checked radiologically. When hyperventilation was used to control ICP, it was set to preserve SjO2>55%. Haemodynamics were monitored using a Swan-Ganz catheter.
None of the patients received antibiotic prophylaxis although antibiotics may have been used to treat diagnosed infections. Febrile episodes were treated at the physician's discretion, using antipyretic drugs or physical therapy.
TEMPERATURES
The ICT was continuously monitored by a silicone intraventricular catheter with a thermistor and a fibreoptic sensor for ICP (110–4HTM Camino Lab, San Diego, CA, USA). The system was screwed onto the skull using a bolt provided by the manufacturer; CSF could be withdrawn through the catheter. In three cases the catheter was positioned intraparenchymally, because of failure in cannulating the lateral ventricles. The catheter was placed in the operating room, under sterile conditions and its correct position was checked by CT at the end of the surgical procedure.
Samples of CSF were collected every 2 days and before removal of the intraventricular catheter for cytochemical analysis and microbiological culture.
Continuous measurements of Tc were taken using a Swan-Ganz catheter (Abbott Critical Care System), with a thermistor positioned 4 cm proximally to the tip. Once the monitoring was discontinued, the accuracy of the two temperature probes (intracranial and core) was checked by an in vitro test on eight intracranial probes and five pulmonary catheters.
The test involved comparing the temperatures provided by the two thermistors with those measured by a precision thermometer (HD 9215, Delta OHM, Padova, Italy). The temperature sensors were immersed in a bath fitted with a thermostat to warm the fluid from 34°C to 45°C and then to cool it. Every 5 minutes the temperatures measured by the two sensors were simultaneously recorded.
DATA COLLECTION AND STATISTICAL ANALYSIS
Intracranial pressure, MAP, and CPP were continuously recorded, sent to a computer through an analog-digital converter (Mac Lab Word Precision Instrument, New Haven, CT, USA) and stored for off line analysis. The signals were analysed using software for Apple Macintosh (Chart 6.3). Temperatures were recorded hourly. Data were summarised as means (SD). The paired t test was used to assess differences between groups. A value of p⩽0.05 was considered statistically significant. The reliability of the temperature sensors was assessed as suggested by Bland and Altman.16
Results
RELIABILITY OF CEREBRAL AND CORE THERMISTORS IN VITRO
A total of 203 paired measurements were obtained for the eight intracranial catheters.
The range was between 33.6°C and 45.0°C. The differences between the measurements with the precision thermometer and the Camino thermistor were calculated. Using the Bland-Altman approach, the mean difference between the two methods and the limits of agreement were determined. The mean difference was −0.05 (SD 0.2)°C; the limits of agreement were between −0.47 and 0.37°C. The same procedure was applied to verify the reliability of the temperature measurements provided by five Swan-Ganz catheters. The mean difference was 0.001 (SD 0.2)°C; the limits of agreement were between −0.4 and 0.4°C.
CLINICAL DATA
Monitoring of ICT was done in 20 patients (10 men) aged between 21 and 78 years (mean 52.7 (SD 18)). Ten had traumatic brain injury (TBI), eight subarachnoid haemorrhage, and two cerebral tumours.
In 17 patients (85%) the catheter was positioned in the ventricular system, in three in the cerebral parenchyma. On average, monitoring started 53 hours (range 2–168 hours) after the injury (TBI), after the first bleeding (SAH), or after surgery. The mean duration of monitoring was 161 hours (range 78–288 hours).
In two patients a small intraparenchymal haemorrhage related to the catheter was discovered, but it did not require surgical intervention. In two patients a meningeal infection was diagnosed.
Table 1 provides summary data of the intracranial parameters and severity for each patient.
Summary data for severity and main intracranial parameters
INTRACRANIAL AND CORE TEMPERATURE
A total of 2477 ICT and 2007 Tc measurements were obtained. Temperatures and their main differences are reported in table 2. Figure1 illustrates the time course of ICT and Tc. Mean ICT was 38.4 (SD 0.8)°C, and mean Tc was 38.1 (SD 0.8)°C. In 1805 cases (73%) ICT was ⩾38°C, and Tc was ⩾38°C in 1154 cases (57.5%). The mean difference between ICT and Tc was 0.3 (SD 0.3)°C (p=0.0001). Out of the 2007 Tc measurements, only 243 (12%) were higher than the corresponding ICT and in 157 cases (7.8%) the two temperatures were the same.
Summary data of temperatures and discrepancies between intracranial temperature (ICT) and core temperature (Tc)

Time course of ICT and Tc.
The differences between ICT and Tc varied widely, both among different patients and in different phases of a single patient's clinical course. The difference, calculated as ICT−Tc, ranged between +2.3°C and −0.7°C. Figure 2 shows the behaviour of ICT and Tc in patient A and patient B during 24 hours. The relation between ICT and Tc in patient B is the one most commonly encountered, ICT being constantly higher than Tc. The relation between the two temperatures is different in patient A, ICT always being lower than Tc, presumably because of the lack of the bone flap that was not reinserted after removal of a subdural haematoma.

Behaviour of ICT and Tc in two patients: The first (A) with an intact skull, the second (B) with a large area of bone decompression.
The differences between ICT and Tc (ICT−Tc) were similar in patients with SAH and SHI, being respectively 0.33 (SD 0.3)°C and 0.32 (SD 0.3)°C (p>0.05).
Because patients with SAH were those in whom CSF was aggressively drained, it follows than CSF drainage did not significantly influence the difference between ICT and Tc.
The severity of the impairment of consciousness did not seem to be related to the difference between ICT and Tc, which was 0.33 (SD 0.28)°C in patients with GCS⩽8 after stabilisation and 0.39 (SD 0.4)°C in patients with GCS>8. As shown in table 2, ICT and Tc sometimes differed widely even in the same patient.
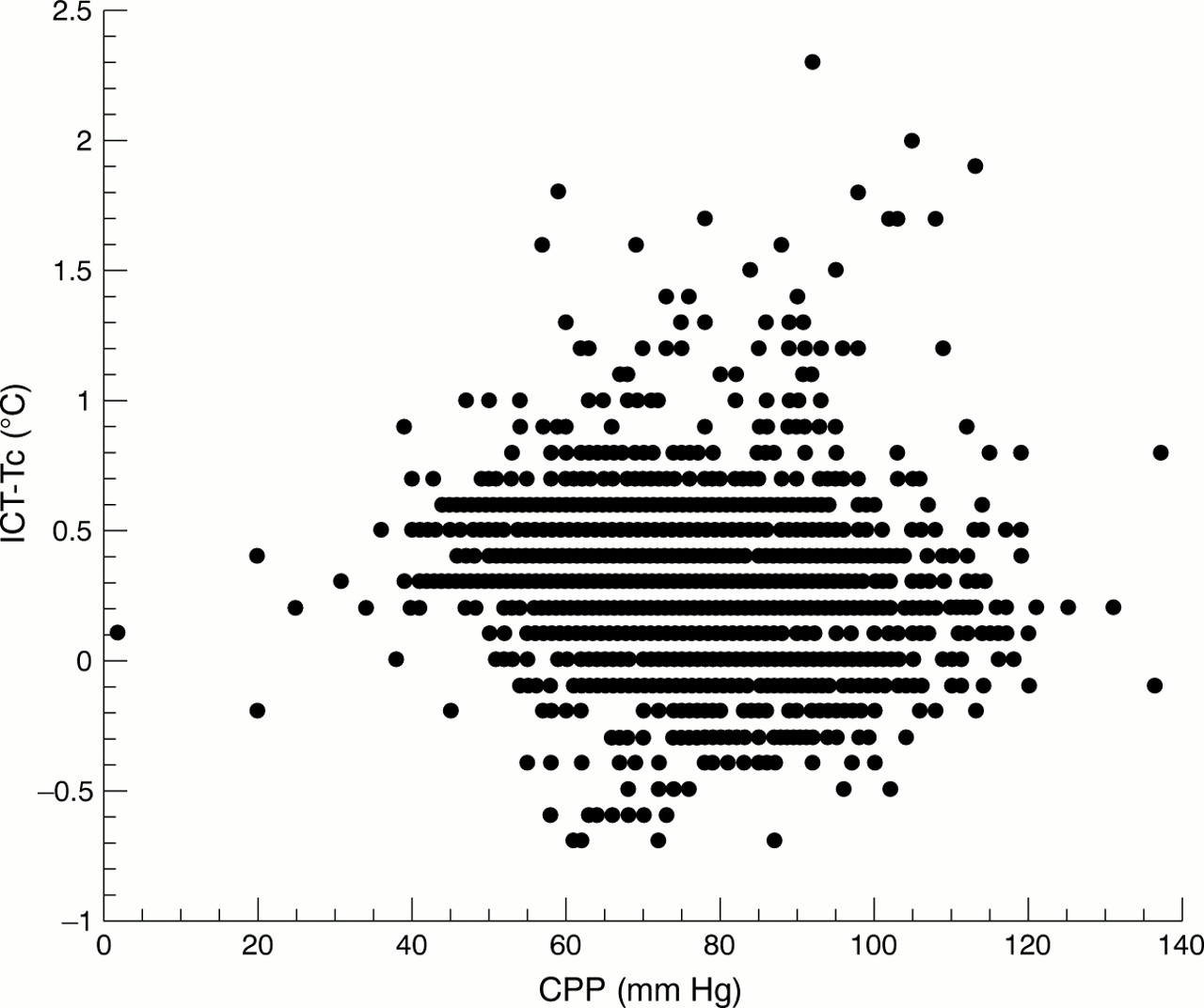
It has been suggested that a reduction in cerebral blood flow (CBF) may affect cerebral temperature and its difference from Tc. Figure 3 shows CPP (taken as an estimator of CBF), plotted against the difference between ICT and Tc. No relation was found. Only at the time of brain death, when CPP was abnormally low, did the differences between cerebral and systemic temperature almost disappear, confirming a previous report.17

Scatter plot illustrating the relation between cerebral perfusion pressure (CPP), taken as an estimator of cerebral blood flow, and the difference between ICT and Tc. CPP values<40 mm Hg were recorded from patients just before and during brain death. When CPP falls the difference between the two temperatures disappears.
During the clinical course the main cause of the differences between ICT and Tc seemed to be changes in body core temperature: 240 episodes (temperature change⩾0.7°C) were identified, coinciding respectively with the onset or resolution of a febrile episode. In 119 cases the temperature rose, and in 121 it fell. The difference between ICT and Tc became significantly larger with the rise in body core temperature and dropped significantly when it fell. The mean difference between ICT and Tc was 0.16 (SD 0.31)°C before febrile episodes (ICT being higher than Tc), and 0.41 (SD 0.38)°C at the febrile peak (p<0.05). This pattern was mirrored while body core temperature fell from the peak: the mean difference between ICT and Tc was 0.37 (SD 0.31)°C at the peak of fever and 0.15 (SD 0.38)°C as it ebbed. When the differences between ICT and Tc was averaged for each patient, the same behaviour was confirmed in most patients (fig 4) (p<0.05).

Left panel: mean differences between ICT and Tc before (A) and at the peak (B) of 119 febrile episodes recorded in 20 patients. One line represents one patient (p<0.05). Right panel: mean differences between ICT and Tc at the peak (A) and after (B) 121 febrile episodes (p<0.05).
BRAIN TEMPERATURE AND ICP
The mean ICP, with the maximum values for each patient, are shown in table 1.
There was no relation between ICP and the absolute value of ICT. However, when changes in temperature were considered, rather than the absolute values, temperature seemed to have a strong effect on ICP. We identified 240 changes in ICT of at least 0.7°C (119 rises and 121 decreases). Figure 5 shows the significant increase in ICP associated with the 119 increases in fever (p<0.001). This behaviour was confirmed even when ICP and ICT were averaged for each patient. The ebb of fever was associated with a significant fall in ICP, from 17.5 (SD 8.62) mm Hg to 16 (SD 7.76) mm Hg (p=0.02).

Box plot showing ICP before the onset of fever (ICP 1)and at the peak of febrile episodes (ICP 2). Median, confidence intervals, middle half of the data between the 25th and 75th percentile, and ranges are summarised (p<0.05).
JUGULAR VENOUS OXYGEN SATURATION AND ICT
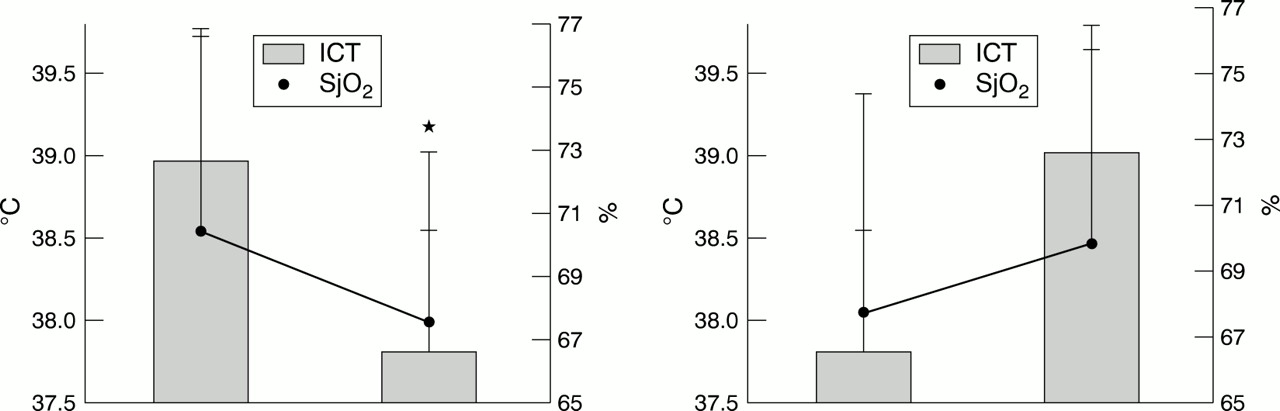
In 10 patients with intermittent monitoring, 133 samples were obtained. In five patients continuous fibreoptic monitoring was performed. Mean jugular venous oxygen saturation in the whole sample was 71.1 (SD 7.0)%. Six episodes of SjO2 desaturation (SjO2<55%) and 119 supranormal episodes (>75%) were detected. No relation could be found between ICT changes and intermittent SjO2 measurements. The relation between febrile episodes and SjO2 was therefore studied in the five patients with SjO2 monitoring. In 71% (15 out of 21 events recorded) SjO2 rose as ICT increased (p=0.21). In 60% (12 out of 20 events), it decreased as ICT fell (p<0.02, fig 6). PaCO2 did not change significantly when SjO2changed.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean SjO2 changes at the ebb (left) and flow (right) of fever. The error bars indicate SDs (*p<0.05).
Discussion
Under normal conditions, the temperature of the brain is dependent on three main factors: local heat production, cerebral blood flow, and the temperature of the blood perfusing the brain. The brain is a big consumer of energy and a big producer of heat, which is not easily dispersed because of the insulation provided by the skull. The brain uses about 20% of the oxygen and 25% of the glucose required by the body at rest (when it weighs only 2%-3% of the total body weight). It has been assessed that of the carbohydrate consumed by the brain, 95% undergoes oxidative metabolism; 43% of the energy originally held in glucose is captured by the ATP, and the remainder is given off as heat.18 On account of its high metabolic activity, cerebral tissue normally produces a considerable amount of heat. Continuous monitoring of brain temperature was originally done by introducing a thermocouple into an intraventricular catheter for intracranial pressure monitoring.19 Today, thermometers or thermistors are combined with other probes (for measuring ICP, oxygen, and other metabolites) so that brain temperature can be measured continuously in the lateral ventricles or in the parenchyma. These techniques have brought to light differences in different areas of the brain, the deeper zones being warmer than the surface structures.20
In our population a consistent difference was found between cerebral temperature and internal body temperature, confirming previous reports.17 19 21 22 In most patients brain temperature was higher than body core temperature. The differences measured were quite large, varying between different patients and between different phases of the clinical course in the same patient. It is still not clear why such differences exist, but a relation has been suggested between cerebral metabolism and the size of the difference between brain and systemic temperatures. Mellergard et al found a smaller difference during impairment of consciousness and in the night in conscious patients, suggesting that the depression of metabolism in coma and—to a different extent—during sleep may lower the brain temperature.23 Other authors have investigated how different CBF levels affect the ICT-Tc gradient.
Rumana et al found that the difference was more marked when CPP was reduced to between 50 and 20 mm Hg, indicating impaired CBF; nevertheless with CPP<20 mm Hg, indicating irreversible impairment of CBF, the difference almost disappeared.17These data were taken to confirm that arterial blood flow achieves a sort of “wash out” of the heat generated by brain metabolism.
Our sample presented considerable between patient differences in brain and systemic temperatures, and this could only be partially predicted from the above factors. The difference between core and brain temperatures could not be explained by the level of impairment of consciousness or the adequacy of the CPP. Only in cases of impending brain death did the brain-core gradient almost disappear.
Even aggressive CSF drainage (which can be reasonably expected to subtract heat from the intracranial space), done in cases of acute hydrocephalus due to subarachnoid haemorrhage, had no effect on the amplitude of the brain−core temperature difference.
The only factor that unquestionably affected the difference between ICT and Tc in our sample was the lack of part of the skull because of bone decompression, which presumably facilitated heat dispersion.
Between patient differences are seen in the brain-systemic temperature gradient. During the clinical course the main cause of the differences between ICT and Tc seemed to be body core temperature. The gap between ICT and Tc increased significantly as body core temperature rose and narrowed significantly as it fell. We can only suggest that cerebral metabolism increases more than systemic metabolism due to the rises in temperature; this pattern was mirrored while the temperature was falling. Tc may thus markedly underestimate brain temperature while the fever is rising. This becomes particularly important in the clinical setting. Pyrexia was in fact extremely frequent in our group of patients: 73% of ICT measurements were 38°C or higher and 85% of the patients had a mean ICT greater than 38°C during the whole monitoring period. Moreover each patient experienced at least one episode of ICT greater than 38°C and 85% had a maximum ICT greater than 39°C.
Our sample is probably too small to be considered representative of the entire population of acute neurosurgical patients, although fever (due to infections or other causes) was one of the major problems in this. There is very little published information about the incidence of fever after acute cerebral damage, although Jones et al confirm these findings.13 The figures for the frequency of fever in a multicentre study enrolling 111 patients with head injury are also in agreement.24
As we mentioned, we were not able to find any relation between the absolute brain temperature and the absolute ICP, which is probably affected by the sum of many factors (primarily intracranial). However, there was a significant relation between the occurrence of febrile episodes and increases in ICP, indicating that temperature instability may be an important cause of derangement of intracranial homeostasis.
From our SjO2 data (which are good indicators of the balance between CBF and metabolism), the increases in ICP associated with increases in temperature seem to be explained by a high temperature increasing CBF more than the cerebral metabolic rate for oxygen (CMRO2). This mismatch is reflected in the increase in SjO2. A change in the opposite direction (CBF reduced more than CMRO2) should be seen when the temperature drops, as SjO2 falls with fever. As we could not measure CBF during temperature changes and we had continuous SjO2monitoring in only five patients, our findings need to be corroborated by further investigations.
However, there are many experimental and clinical reports of an increase of the ratio of CMRO2 to CBF when body temperature drops, reaching hypothermia.10 11 25 A change in the opposite direction has been described during the rewarming phase. These findings are in the same direction as ours. Therefore, our SjO2 data indicate that the increase in ICP seen at the same time as the increase in brain temperature may be sustained by a rise in cerebral blood volume.
Conclusions
Fever is extremely frequent after acute cerebral damage and cerebral temperature is significantly higher than body core temperature. Body core temperature may markedly underestimate cerebral temperature, especially during the phases when temperature has the greatest impact on the CNS. We found that rises in temperature are associated with derangements of intracranial volume homeostasis documented by increases in ICP. From an analysis of SjO2, this increase in ICP seems to be explained by the fact that changes in temperature affect CBF more than the metabolism of oxygen.