Article Text

Abstract
Background and objective In current clinical practice, old patients with stroke are less frequently admitted to neurorehabilitation units following acute care than younger patients based on an assumption that old age negatively impacts the benefit obtained from high-intensity neurorehabilitation. Our objective was to test this assumption empirically in a large sample of patients with stroke.
Methods Functional recovery during 4 weeks of inpatient neurorehabilitation was assessed with the Barthel Index (BI) in 422 middle-aged (<65 years), 1399 old (65–80 years) and 473 very old (>80 years) patients with stroke. Overall functional recovery, recovery patterns and the relationship between therapy intensity and recovery were statistically compared between the three age groups.
Results Overall functional recovery was statistically equivalent in middle-aged, old and very old patients (average improvement in BI total score: middle-aged: 15 points; old: 15 points; very old: 14 points). A novel item-wise logistic regression analysis (see Pedersen, Severinsen & Nielsen, 2014, Neurorehabil Neural Repair) revealed that this was true for 9 of the 10 everyday functions assessed by the BI. Furthermore, functional recovery was predicted by the amount of therapy (R=0.14; p=0.0001), and age did not moderate this relationship between therapy intensity and recovery (p=0.70).
Conclusions Old and even very old patients with stroke benefit from specialised inpatient neurorehabilitation and high amounts of therapy in the same degree as younger patients. Contrary to current clinical practice, old age should not be a criterion against admission to a neurorehabilitation unit following acute stroke treatment.
- STROKE
- REHABILITATION
- CLINICAL NEUROLOGY
- EVIDENCE-BASED NEUROLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Global increases in age and stroke rates combined with better acute stroke treatment leave more and older patients with residual impairment after acute stroke.1 ,2 Older patients have worse prestroke status, greater impairment on hospital admission, more comorbidities and show poorer functional status after acute stroke treatment than the younger patients.3–5 Older patients with stroke are also admitted to neurorehabilitation units less often than younger ones.6 ,7 Why old patients should receive the same treatment during the acute phase but different subacute therapy than younger patients is unclear, particularly since neurological treatment followed by specialised neurorehabilitation reduces 1 year mortality by 40% and more than doubles functional recovery relative to general medical treatment.8–10
There is the occasional assumption that elderly patients do not benefit from or cannot participate in high-intensity neurorehabilitation as the younger patients and should, therefore, be referred to less therapy-intensive and cost-intensive settings.11 However, the empirical evidence for this assumption is limited; some investigations found an effect of age,12–14 but others did not.15–17 Moreover, a major limitation of previous empirical research on this topic is that studies have used change in total scores on the functional independence measure (FIM) or on the Barthel Index (BI) to quantify functional recovery. While total scores on these measures are good indicators for overall dependency of care, these do not carry information about independence within each of the assessed functional domains and therefore, can conceal diversity in recovery patterns.18 To address these gaps in current evidence, we analysed data from a several fold larger cohort (n=2294) than previous studies and tested (1) if age modulates overall functional recovery during high-intensity inpatient neurorehabilitation as assessed with the BI total score; (2) if age affects the relationship between therapy intensity and overall functional recovery, in other words, if the benefit obtained from each administered hour of neurorehabilitative therapy differed between middle-aged, old and very old patients; and (3) if age influences recovery in specific domains of everyday functioning, using an item-wise analysis recently developed by Pedersen et al.18
Materials and methods
A systematic analysis of the Meerbusch Registry, a prospectively maintained database of all patients admitted to the Neurological Rehabilitation Department of the Mauritius Hospital in Meerbusch, Germany, was conducted. Patients were transferred to our clinic from neurological stroke units and other acute-care departments. Anonymised data from patients who met the following inclusion criteria (n=3021) were extracted from the Meerbusch Registry: (1) one of following diagnoses from the 10th version of the International Classification of Diseases (ICD-10): I63 or I64; and (2) inpatient stay of at least 4 weeks in the years 2008–2012.
All patients were administered a high-intensity multidisciplinary neurorehabilitation programme, including physiotherapy, ergotherapy and sports-therapy, nurse-delivered activation training, speech and language therapy and neuropsychological training. Therapy was delivered in a modular approach in single or group sessions, as deemed appropriate. Within each module, multiple evidence-based treatment options were provided, which were arranged in cycle-training clusters and combined according to individual needs to achieve high specificity of treatment.19
The functional status of patients was assessed using BI on admission and at regular intervals throughout the inpatient stay (at least once per week). The BI is a broadly-used and well-validated clinicometric tool with high inter-rater and test retest reliability.20 ,21 The BI addresses 10 categories of activities of daily living (eg, mobility, dressing, toilet use), for which the degree of independence is rated. The highest possible score is 100, the lowest 0. The assessment was carried out by trained nursing staff and was based on actual daily, rather than on rare and short-lived, performance. Patients with incomplete records of the BI were excluded from statistical analysis. This resulted in a final sample size of 2294 patients (figure 1).

Sample selection process.
For statistical analysis, each patient was classified into one of three age groups: (1) patients under the age of 65 years (n=422), (2) patients aged 65 to 80 years (n=1399), and (3) patients over the age of 80 years (n=473). These age groups were chosen based on sociocultural convention and we refer to them as ‘middle-aged’, ‘old’ and ‘very old’, respectively. Since length of stay in inpatient neurorehabilitation varied across our patients, statistical analyses focused on functional recovery over a fixed period of 4 weeks.
Three sets of statistical analyses were conducted. The first analysis tested whether functional recovery during neurorehabilitation differed between the age groups. Functional recovery was quantified as the improvement in functional status over the 4 weeks interval, that is, the difference in the BI at admission and in the BI after 4 weeks of inpatient stay.i A One-Way analysis of variance (ANOVA) on functional recovery, with age group entered as a between-subject factor (3 level), was calculated. Pairwise follow-up comparisons of age groups were conducted using Games-Howell post hoc tests, respectively. While existing evidence on the effect of age is inconclusive, with equivalent and non-equivalent recovery being reported in previous studies, we note that those investigations that did not find an effect were typically conducted in larger samples and clearly distinguished between functional recovery and functional status. Therefore, we expected that functional recovery would not depend on age, and complemented the ANOVA for functional recovery by statistical equivalence testing, using the method by Rusticus and Lovato22 for designs with multiple groups. This analysis tests whether CIs for group differences fall within a predefined equivalence interval. 95% CIs were calculated for each pairwise comparison using Games-Howell post hoc tests (which account for unequal group sizes and violations in homogeneity of variance). The equivalence interval was defined as ±5 points on the BI, which we consider a very stringent criteria (for comparison, see eg, refs. 23 and 24).
The second set of analyses assessed the relationship between overall functional recovery and therapy intensity, and tested whether this relationship differed between the age groups. While all patients in our study took part in a multidisciplinary rehabilitation programme with similar components and intensity, there was nonetheless some variation in the amount of therapy hours administered to each patient. We extracted the amount of therapy hours from the electronic records for each patientii and calculated two linear regression models. The first model tested whether the amount of training received during the 4 weeks of inpatient stay significantly predicted functional recovery. The second regression model tested whether the relationship between therapy intensity and functional recovery differed between the three age groups and contained the predictors: therapy hours, age group and an age group x therapy hours interaction term.
The third set of analyses assessed whether age affected recovery in certain functional domains. To answer this question, we adopted an item-wise analytical approach, as recently presented by Pedersen et al18 for the analysis of FIM scores in traumatic brain injury. This approach uses item-wise logistic regressions to test whether the odds of achieving an independent level of functioning for each assessed item is dependent on age. To conduct this analysis, scores for each BI item after 4 weeks of neurorehabilitation were first dichotomised. If a patient achieved the maximum score on a given item, this was coded as ‘independent’ (1), else it was coded as ‘dependent’ (0). Next, logistic regressions were calculated for each item to test whether age group (categoricaliii) and therapy hours predicted the functional outcome (independent/dependent). These regressions were adjusted for the functional status on admission by adding two further predictors: (1) item-specific BI score on admission, and (2) overall functional status on admission (quantified as the number of other items with an ‘independent’ score at admission). In other words, these regressions test whether the prognosis for functional recovery during 4 weeks of neurorehabilitation, corrected for the functional status at admission, is different for middle-aged, old and very old patients.
The fit of the item-wise logistic regression models was assessed by the Hosmer-Lemeshow goodness-of-fit tests and the Nagelkerke R2. Model fit was adequate (Hosmer-Leweshow p>0.05) for all items, except for the items Bladder control and Feeding. Average R2 was 0.58 (range: 0.38 (Stairs) to 0.70 (Bowel Control)), indicating that these rather simple models could account for a considerable proportion of the variation in the functional outcomes.
All statistical analyses were conducted two-tailed with α set at 0.001 and were computed using SPSS (V.22, IBM Corporation).
Results
Equivalent overall functional improvement in the three age groups
Overall functional improvement over 4 weeks of inpatient neurorehabilitation, defined as the change in BI score from admission, did not significantly differ between the age groups (One-Way ANOVA, F=0.87, df=2, p=0.42). Middle-aged and old patients improved by 15 points on the BI on average; very old patients by 14 points (figure 2).
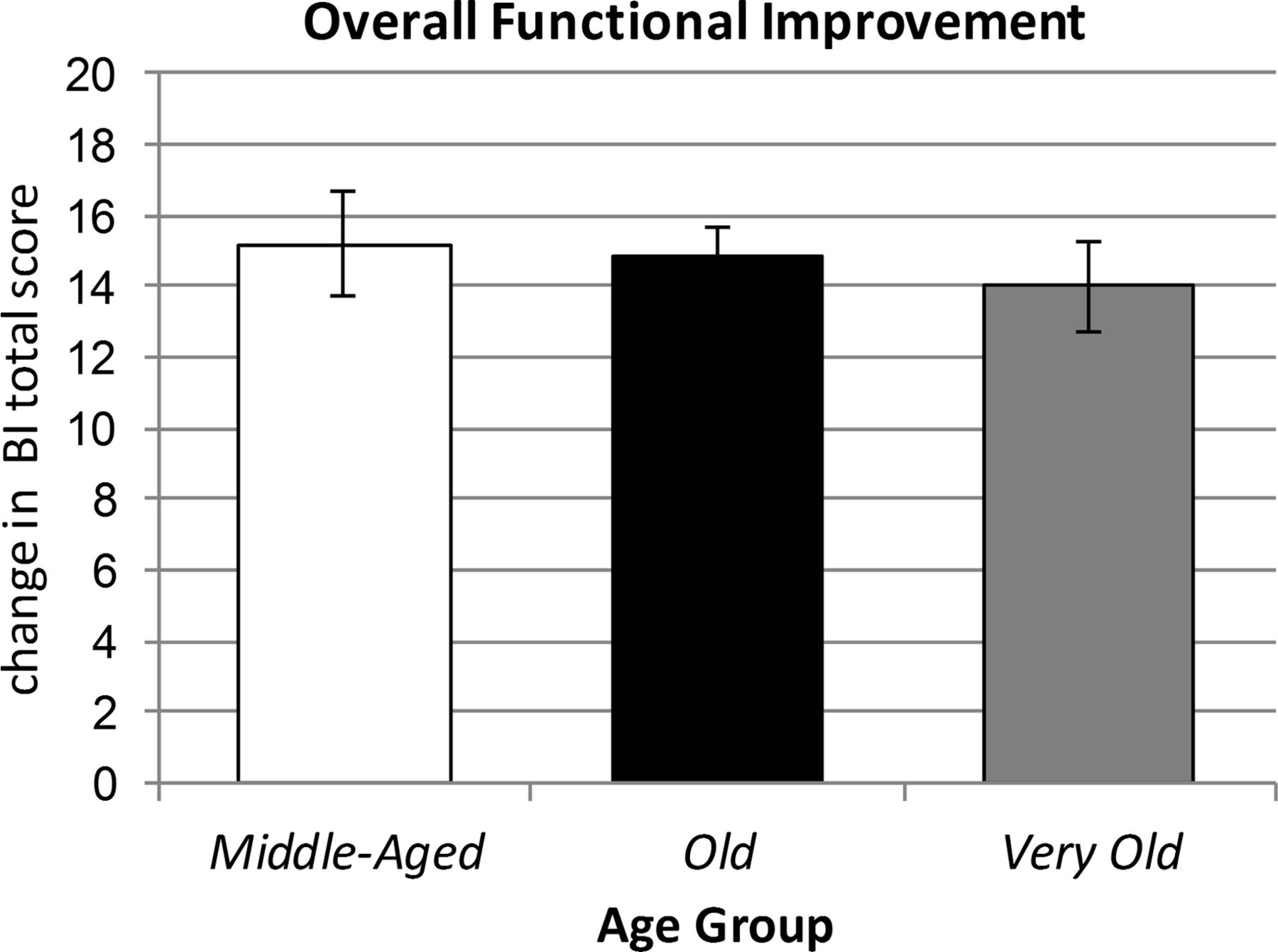
Average functional improvement (change in total score on Barthel Index (BI)) over 4 weeks of in-patient neurorehabilitation. Error bars represent the 95% CI.
Thus, all three age groups showed a comparable functional improvement and appear to have profited equally from the neurorehabilitation therapy. To corroborate this conclusion, we conducted statistical equivalence testing for each pair-wise comparison. The results of the equivalence testing are presented in table 1. The CIs for all pair-wise comparisons fell within the equivalence interval. Therefore, statistical equivalence of the functional improvement in the three age groups was confirmed.
Pair-wise comparisons of the functional improvement in the three age groups
Therapy intensity and overall functional improvement
The amount of therapy received during the 4 weeks stay significantly predicted functional recovery (R=0.14, F=47.88, p=0.0001). This relationship between the hours of therapy and functional recovery was not significantly influenced by age group (therapy hours×age group interaction term: F=0.36, p=0.70), and adding the factors age group and age group×therapy hours to the regression model did not significantly improve the model (change in R2=0.001, p=0.78). In summary, functional recovery was weakly but significantly related to the therapy amount, and this relationship between therapy intensity and recovery did not significantly differ between middle-aged, old and very old patients.
Age and improvement in the different functional domains
We used item-wise logistic regressions18 to test for potential age-group differences in the recovery of each of the 10 functional domains assessed by the BI. The regression tested whether the odds of achieving an independent level of function for a given domain (ie, achieving a maximum score on the corresponding BI item) is dependent on age, and were corrected for the domain-specific and overall functional status at admission and administered therapy hours.
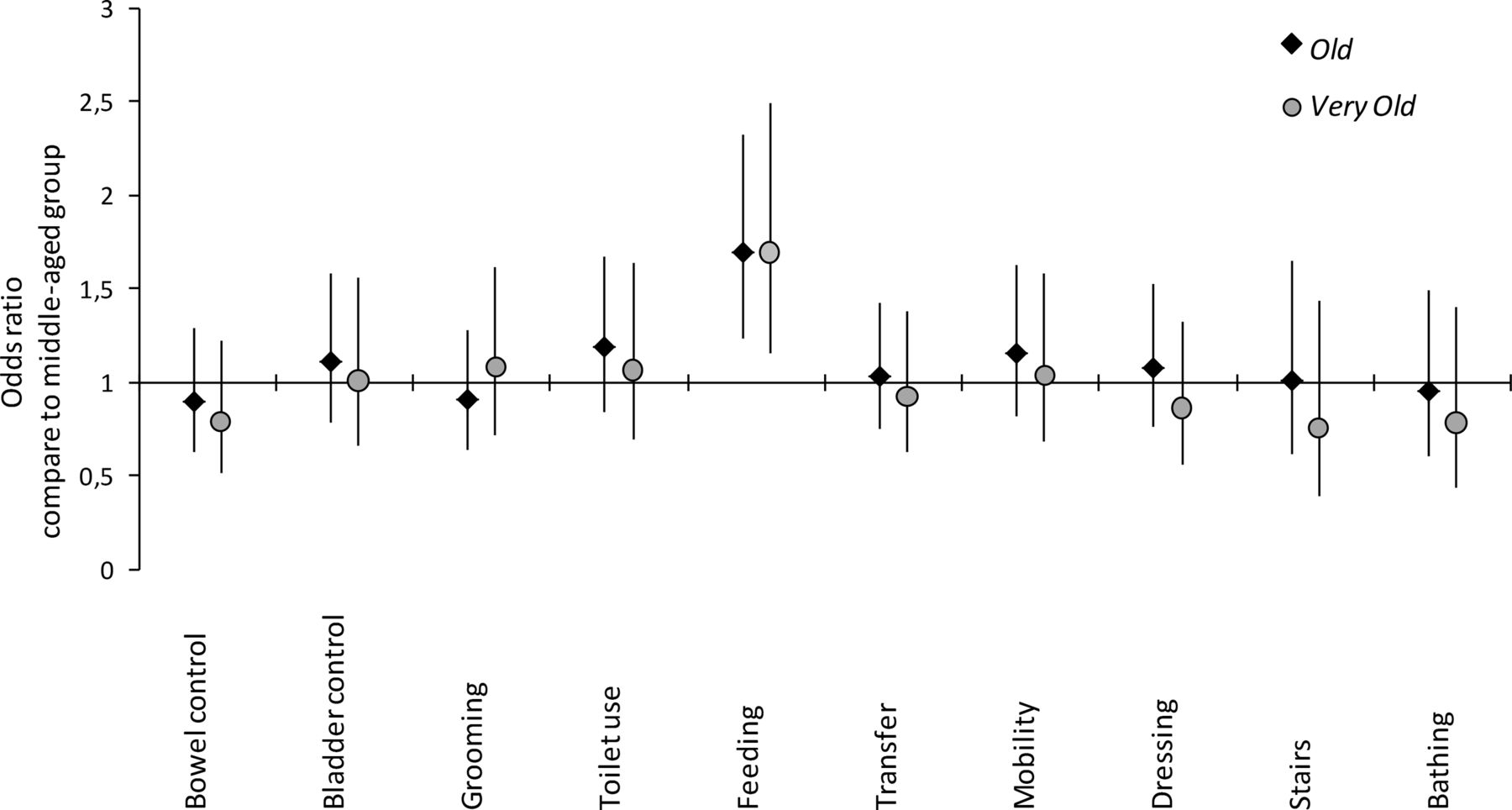
Like overall recovery, recovery in the different functional domains was very similar across the three age groups. For 9 of the 10 functional domains, no significant effect of age group was found in the item-wise logistic regressions (all p’s>0.29). In other words, when controlled for functional status on admission and administered therapy hours, the odds of old and very old patients to achieve independence in the different functional domains did not differ from the odds of middle-aged patients (figure 3 for details). The analysis of the item Feeding did show a significant effect of age group, such that recovery was greater for old and very old patients than middle-aged patients (ORs: old vs middle-aged=1.69, 95% CI 1.23 to 2.32, p=0.001; very old vs middle-aged=1.80, 95% CI 1.15 to 2.49, p=0.007). However, given that the model fit was poor for this particular analysis (Hosmer-Lemeshow-test: p=0.005), this finding should be interpreted with caution.

{kind=link}
{kind=link}
{kind=link}
Between-age-group OR for achieving functional independence in each of the 10 Barthel Index items, adjusted for functional status on admission and therapy hours. The graph represents the adjusted odds of old (black diamond) and very old (grey circle) patients to achieve functional independence in comparisons to the odds of middle-aged patients. A value of 1 means that the odds of the older age groups are identical to those of the middle-aged group. The prognosis for old and very old patients was comparable to the prognosis of middle-aged patients for 9 of the 10 items, and even significantly better for the item feeding. Error bars represent the 95% CI.
Discussion
The current study assessed the impact of age on functional recovery during high-intensity neurorehabilitation following stroke. Three main findings were obtained. First, middle-aged, old and very old patients showed an equivalent overall functional recovery during 4 weeks of inpatient neurorehabilitation. In other words, while very old patients had a lower functional status both on admission and after 4 weeks, middle-aged, old and very old patients gained an equivalent amount of functional independence during neurorehabilitation. Second, the extent of overall functional recovery was predicted by the amount of therapy patients underwent, independent of age. Third, a novel item-wise analysis revealed that recovery in the different functional domains assessed by the BI did not significantly differ between the age groups either, that is, middle-age, old and very old patients showed similar recovery patterns. Taken together, the findings of this study show that (higher) age does not diminish the benefit obtained from specialised, high-intensity neurorehabilitation.
The data obtained from our large sample of patients with stroke converges with three previous studies in smaller cohorts that also did not find any systematic effect of age on functional recovery during specialised neurorehabilitation.15–17 In contrast, others have reported a detrimental effect of age on rehabilitation outcomes in patients with stroke.12–14 ,25 ,26 There are several plausible explanations for this divergence in results. First, many of the studies that did find an effect of age on recovery were conducted in small samples.12 ,13 ,25 Sample size is a key determinant of the statistical power of a study and low-powered studies overestimate the magnitude of effects and suffer from reduced positive predictive value.27 Second, two previous studies concluded that older age negatively impacted recovery on the basis that old patients were less likely to achieve a predefined ‘success score’ on the BI26 or FIM12 at discharge from neurorehabilitation. These observations do not conflict with our data; we also find that functional independence after 4 weeks of neurorehabilitation was lower in very old patients compared to middle-aged and old patients. Importantly, however, our current and previous data15 ,16 show that this age effect disappears when the functional status of the patient at admissions is accounted for. Third, the divergence in results could be explained by differences in rehabilitation protocols and settings. Finally, in line with a recent meta-analysis,28 our data corroborate that recovery is positively correlated with therapy intensity. A fourth potential explanation could be that an apparent detrimental effect of age on recovery in previous studies arose as consequences of unobserved or unaccounted differences in the amount of therapy administered to older versus younger patients within the same treatment unit.
An important extension of the current compared to previous studies on the impact of age on recovery following stroke is that we complemented analyses of the overall functional improvement, as quantified by the BI total score, by item-wise analysis. This recently developed analysis technique has two main advantages.18 First, unlike standard multiple regression analysis or non-parametric rank analysis, it is not compromised by violations of interchangeability of items (which have been reported for the BI29). Second, arguably even more importantly, this item-wise analysis provides a more detailed picture of the recovery patients undergo as it is sensitive not only to changes in overall functions, but also to patterns or shifts in functional domains.
There was one exception to our general finding that age did not impact recovery: the item-wise regression for Feeding indicated that the odds of achieving an independent level of function in this domain were higher in old and very old patients compared to middle-aged patients, suggesting that recovery in this functional domain was actually greater in older compared to younger patients. However, we note that the model fit was poor for this particular item, indicating that this result might not be very reliable. Future studies might investigate recovery in this function of everyday life in more details.
A limitation of the present study is that referral criteria for neurological rehabilitation were discretionary. Therefore, residual bias for referral of patients with stroke with less comorbidity compared to the population average cannot be fully excluded. Further, we note that our study did not assess the neurobiological mechanisms underlying functional recovery; therefore, the current data does not state whether age might impact how functional recovery is achieved.
The discussion about the most appropriate rehabilitative setting for elderly patients with stroke often refers to health economics. Resource-intense neurorehabilitation in older patients might appear cost-ineffective because the limited life-expectancy of old people does not provide enough payback time in terms of savings in nursing needs. The BI constitutes a good measure for dependency on everyday care and for economic impact, and therefore our findings can help inform this discussion. For instance, Caro et al30 showed that a 15 point difference in the BI, as observed in our neurorehabilitation cohort, corresponds to a 30% reduction in stroke-related costs. Similarly, O'Connor et al31 calculated that the average payback time for 59 days of inpatient neurorehabilitation (with an average improvement of 34 points on the BI) in terms of savings in postrehabilitative nursing care is 21 weeks. On the basis of their calculation and assuming linear effects for a stay of 28 days with an average improvement of 15 points on the BI, as in our study, the payback time for high-intensity neurorehabilitation for patients older than 80 years is less than half a year. From a purely economic point of view, our findings therefore indicate that all patients with a remaining life expectancy of half a year or more should be admitted to high-intensity neurorehabilitation because it will save money for society.
Conclusions
Old and very old stroke-patients benefit from high-intensity neurorehabilitation to the same degree as younger/middle-aged patients. Contrary to current clinical practice, higher age should not bias decisions about admission to specialised neurorehabilitation units following acute stroke treatment.
Acknowledgments
The authors would like to thank W Schicks for his helpful support in retrieving the data for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors All authors conceived the study. BS and JR conducted the data analysis. SK, JR, K-MS and BS interpreted the data. SK, JR and BS wrote the manuscript. All authors contributed to the critical revision of the manuscript before publication. All authors had access to the anonymised data and statistical reports included in this study, and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This research was supported by intramural funding of the Mauritius Hospital, Meerbusch.
Competing interests SK, JR, K-MS and BS have received support from the Mauritius Hospital for the submitted work; MU and KB have no financial or non-financial interests that may be relevant to the submitted work.
Ethics approval Based on current legislation in North-Rhine Westphalia, Germany (§15, Berufsordnung für die nordrheinischen Ärztinnen und Ärzte), approval from an ethics committee was not sought for this retrospective analysis of anonymised non-identifiable, non-biological data.
Provenance and peer review Not commissioned; externally peer reviewed.
↵i A complementary analysis of functional status at admission and after four week of inpatient stay can be found in the online supplementary material.
↵ii Nurse-delivered training (eg, in activities of daily living) was not considered in this computation as it was not recorded electronically.
↵iii All regressions were also calculated with age (in years) as a continuous predictor, with all results qualitatively unchanged.