Article Text

Abstract
Background The aim of this study was to determine the strength of the association between intracerebral haemorrhage (ICH) and cerebral amyloid angiopathy (CAA) in a systematic review of published neuropathological studies.
Methods In April 2011, Ovid Medline (from 1950) and Embase (from 1980) were searched for neuropathological studies that quantified the prevalence of CAA in patients with ICH and in a control group without ICH. Two authors extracted data from each study and meta-analysed their results using a random effects model.
Results 10 neuropathological cross sectional or case control studies were identified, involving 481 cases with ICH and 3219 controls. There was no association between CAA and ICH in any location (OR 1.21, 95% CI 0.87 to 1.68; 10 studies, I2 29%), deep ICH (OR 0.81, 95% CI 0.30 to 2.19; five studies, I2 58%) or cerebellar ICH (OR 2.05, 95% CI 0.55 to 7.63; four studies, I2 0%). CAA was significantly associated with lobar ICH, both overall (OR 2.21, 95% CI 1.09 to 4.45; six studies, I2 40%) and in the three studies where average ages for cases and controls were comparable (OR 3.24, 95% CI 1.02 to 10.26).
Conclusions There is an association between CAA and lobar ICH, although the association might be stronger if potential confounding factors, distinctive clinical and imaging features of ICH due to CAA and CAA neuropathological severity are taken into account.
Statistics from Altmetric.com
Introduction
During the past decade, spontaneous (non-traumatic) intracerebral haemorrhage (ICH) accounted for ∼10% of strokes in high income countries and ∼20% of strokes in low/middle income countries, where the 1 month case fatalities were 25–35% and 30–48%, respectively.1 Although time trends have varied between regions, the case fatality 1 month after ICH has remained ∼40% across the globe during the past few decades.2 Understanding that systemic arterial hypertension is the strongest modifiable risk factor for ICH led to trials of secondary prevention with antihypertensive drugs,3 4 which appear to improve outcome for survivors of ICH (regardless of its location).5 Further improvements in outcome could arise from a better understanding of the causes of ICH. Because survivors of lobar ICH appear to be at a higher risk of recurrent ICH than survivors of deep ICH,6 the causes of lobar ICH are of particular interest.
The deposition of β-amyloid peptide in the media of cortical and leptomeningeal arteries, arterioles and capillaries—now known as cerebral amyloid angiopathy (CAA)—was first identified in the early 20th century.7 8 CAA is quite prevalent in cognitively unimpaired elderly people and even more prevalent in those with dementia.9 Since the late 1970s, influential case series have suggested that CAA may cause lobar ICH.10 11 However, in everyday clinical practice,12 CAA is often inferred to be the cause of lobar or cerebellar ICH, especially if the patient is elderly, the ICHs are recurrent or multifocal or haem sensitive gradient recalled echo (GRE) MRI sequences demonstrate at least one lobar brain microbleed.13
However, the strength of the overall association between CAA and ICH remains to be precisely quantified (in lobar and cerebellar locations in particular, but also in deep locations),14 so we performed a systematic review and meta-analysis of published neuropathological studies. We aimed to take account of three potential confounding factors that should be described, and preferably controlled or adjusted for in comparisons of cases and controls: first, patient age, given the increasing CAA prevalence with age9; second, cognitive impairment (and its severity), given the greater prevalence of CAA in those with cognitive impairment than in those without dementia9 15; and third, patients' racial origins, given racial differences in the prevalence of apolipoprotein E polymorphisms which have been associated with ICH due to CAA16 17 and racial differences in the proportion of ICH in a lobar location.18
Methods
Search strategy and selection criteria
In April 2011, two authors (NS and RASS) searched Ovid Medline (1950–) and Embase (1980–) using comprehensive electronic search strategies (see supplement for more details, available online only). One author (NS) also searched the bibliographies of relevant publications and Google Scholar for other papers citing each included paper. We also searched the tables of contents of several journals (Journal of Neurology, Neurosurgery and Psychiatry; Lancet Neurology; Annals of Neurology; Brain; Lancet; Neurology; and Stroke) from 2005 and our personal files.
Eligibility criteria
Studies were eligible for inclusion if they had diagnosed CAA on pathological examination of a brain biopsy or autopsy and quantified the prevalence of CAA in patients with spontaneous (non-traumatic) ICH as well as a group of patients without ICH.
Data collection
Two authors (NS and RASS) screened all titles and abstracts for eligibility, removed duplicates and read the full text of articles that were potentially eligible for inclusion. Eligible studies were read in full by two authors (NS, RASS) who extracted data independently on the following: study design, types of cases and controls, methods of assessment and grading of CAA, prevalence of CAA in cases and controls, and whether any confounders were accounted for. We resolved disagreements by discussion. If pertinent study attributes or data were unavailable or unclear in an eligible publication, we sought clarification from the authors by post and email. We also sought individual patient data from included publications—either in person or by email and post—in order to stratify or adjust the analyses for the potential confounding variables of age and comorbid cognitive impairment, as well as to explore the strength of the association between ICH and CAA according to the neuropathological severity of CAA; unfortunately, only one study provided these data, precluding an individual patient data meta-analysis.14
Methodological assessment
NS was guided in her assessment of the methodological quality of the included studies by the Newcastle–Ottawa scale,19 which uses eight items to judge the quality of case control studies on their selection of study groups, the comparability of their cases and controls, and their ascertainment of exposure of cases and controls (ie, to CAA). If a study fulfils the criteria for an item, a score of 1 point is allocated, with the exception of comparability which can score up to 2 points, resulting in a maximum score of 9 points.
Statistical analysis
If we identified multiple publications relating to the same cohort, we included the largest study. For each study, we determined the numbers of cases and controls and the prevalence of CAA in each group. We sought to stratify our analyses by ICH location (deep, lobar, cerebellar or all locations grouped together), age, neuropathological ratings of CAA severity and racial origin of the participants. We meta-analysed the data in StatsDirect statistical software V.2.7.8, using a random effects model with Der Simonian-Laird weights, quantified the strength of any association using OR and its associated 95% CI, and assessed inconsistency with the I2 statistic. In a separate sensitivity analysis, we tested whether the restriction of our analysis to studies explicitly stating that all ICH were non-traumatic changed the direction or strength of the association between CAA and ICH in all locations. In subgroup analyses, we examined the strength of the relationship between CAA and cases with lobar ICH in studies where the average ages of cases and controls were comparable versus those where average ages of cases and controls were dissimilar or unknown, and in studies in which participants were Asian versus those in which they were not.
Results
Our search strategies identified 1824 articles, of which 19 appeared to be eligible (figure 1). We excluded nine studies because they provided insufficient data to quantify the numbers of cases and controls with and without CAA in seven studies,20–26 cases were selected only if they were affected by CAA27 and the remaining study reported data already included in this systematic review.28 We included 10 neuropathological studies involving 481 cases and 3219 controls from China,29 30 Japan,15 31 Chile,32 India,33 Australia34 and Europe.14 35 36

Selection of studies included in the systematic review.
Critical appraisal
We compared included studies to the ideal design for a study of the association between CAA and lobar ICH (box 1) and rated them using the Newcastle–Ottawa scale (table 1).
Ideal design of a pathological study of the association between cerebral amyloid angiopathy (CAA) and spontaneous intracerebral haemorrhage (ICH)1937
Selection of cases and controls
Representative sample of cases, with ascertainment clearly defined
Independent validation of case diagnosis
Clinical features described
Incident cases of ICH, recruited at a specified inception point, described in relation to the time of neuropathological examination
Spontaneous and traumatic ICH distinguished
First ever and recurrent ICH distinguished
Radiological confirmation of ICH diagnosis and its anatomical distribution, using a standardised classification of lobar versus deep ICH (whose interobserver reliability has been assessed)
Appropriate controls
Derived from the same population as cases
Ascertained in the same way as the cases
Without a history of ICH (if cases were first ever diagnoses)
Quantification of eligible cases and controls not included or omitted from analyses
Assessment of CAA
Pathologically confirmed either at tissue biopsy or at postmortem examination
Detected and rated blind to relevant clinical information
Methods of tissue preparation, staining and analysis identical for all cases and controls
Rated according to a standard or externally validated rating scale, and severity specified
Anatomical location specified in relation to ICH
Reporting and analysis
Presentation of summary data, stratified by ICH location, age of person, past history of cognitive impairment
Cases and controls matched for major confounders (ie, age and past history of cognitive impairment) or confounders adjusted for in the analysis
Characteristics of the selection and comparability of cases and controls in the included studies
Selection of study groups
Studies' ascertainment of cases ranged from highly representative samples of deaths in a community to consecutive, randomly sampled or selected hospital autopsies (table 1). Eight studies clearly defined their cases as having spontaneous ICH14 29–33 35 36 and the corresponding author confirmed that ICH cases were spontaneous in another study.34 Five studies stated that the ICH had been clinically symptomatic.14 29 32 33 36 Two studies included both first ever and recurrent ICH35 36 but the remainder did not specify the inception point for ICH cases. Only five studies described the ages of included cases.14 31 32 35 36 Three studies did not systematically specify ICH locations29 30 33 but the remainder did, albeit with different categories (table 1). Furthermore, studies varied in their definitions of ‘lobar’ ICH, including: ICH that had originated in the cerebellum,36 cortex or subarachnoid space31; subcortical, cortical or in the insular cortex closely related to the basal ganglia14; and in another, lobar ICH was distinguished from multiple cortico-subcortical ICH.35
Comparability of cases and controls
All but one study33 described ascertainment of controls from the same population as the cases (consecutive hospital autopsy controls,29 30 34 35 selected hospital autopsy controls14 31 32 36 and community controls),15 such that the controls could have been cases had they been affected by ICH (table 1). In four studies, 16–82% of the control groups had ischaemic stroke.14 31 33 Considering potential confounding factors, two studies included controls with dementia diagnosed on clinical and neuropathological grounds,30 34 35 only five studies described the average ages of their cases14 31 32 35 36 and only four studies described the average ages of their controls,14 31 32 36 but just three studies accounted for confounding by matching the ages of cases and controls within 5 years.14 32 36
Ascertainment of exposure of cases and controls
All but one study36 assessed cases and controls for CAA in the same way (table 2) but only one study32 reported that the assessment was blinded (although the nature of blinding was unclear). The extent of sampling varied between studies (table 2). Eight studies used Congo Red staining to detect CAA,14 15 29–33 36 one of which also used immunohistochemistry in every case.30 The rating of CAA severity involved a variety of rating scales—many of which were bespoke, being devised by the authors themselves (table 2)—and CAA severity in cases and controls was seldom quantified in every patient. Following communication with the corresponding author of one study,14 we established that only four studies described whether CAA was specifically present in the vessels adjacent to the ICH (so that lobar ICH could be attributed to lobar CAA).15 29–31
Characteristics of the assessment of exposure in the included studies
Association between CAA and ICH
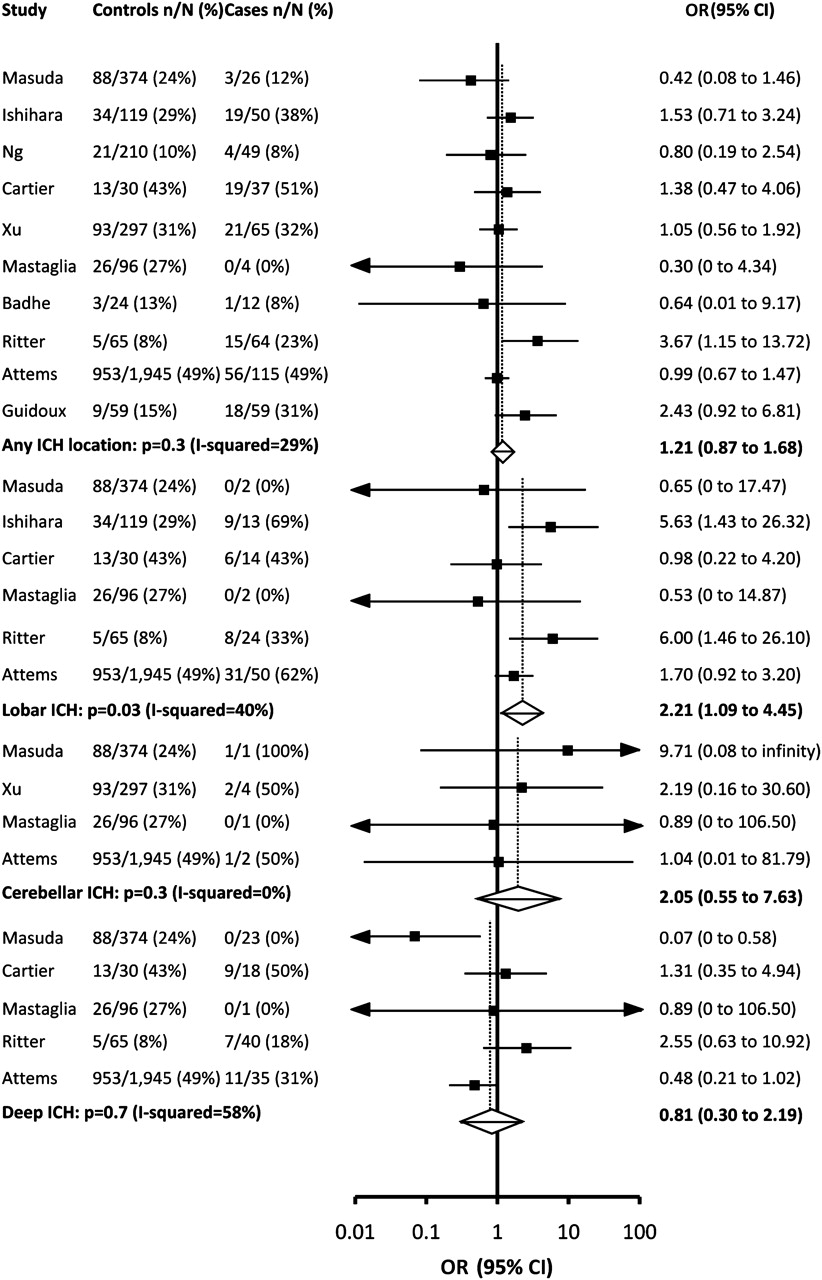
Our meta-analyses did not reveal an association between CAA and ICH in any location in all 10 studies (OR 1.21, 95% CI 0.87 to 1.68; I2 29%; figure 2) nor in a sensitivity analysis omitting one study that might have included traumatic ICH (OR 1.19, 95% CI 0.84 to 1.67).15 There was no significant association between CAA and deep ICH (OR 0.81, 95% CI 0.30 to 2.19; five studies, I2 58%)14 15 32 34 35 or cerebellar ICH, although there were only eight cases of cerebellar ICH (OR 2.05, 95% CI 0.55 to 7.63; four studies, I2 0%).15 30 34 35 However, CAA was more prevalent in lobar ICH cases (54/105, 51%) in comparison with controls (1119/2629, 43%) (OR 2.21, 95% CI 1.09 to 4.45; six studies, I2 40%).14 15 31 32 34 35 In subgroup analyses of the association between CAA and lobar ICH, the association remained in the three studies where the average ages of the cases and controls were comparable (OR 3.24, 95% CI 1.02 to 10.26),14 31 32 but not in those where ages were dissimilar or unknown (OR 1.58, 95% CI 0.91 to 2.77).15 34 35 We could not demonstrate that the association between CAA and lobar ICH was different in studies of Asian patients (OR 3.02, 95% CI 0.44 to 20.77)15 31 or patients of other ethnic origins (OR 1.89, 95% CI 0.86 to 4.15).14 32 34 35
{kind=link}
{kind=link}
OR meta-analysis. Cerebral amyloid angiopathy prevalence in cases with intracerebral haemorrhage (ICH) (stratified by location) versus controls. Squares are point estimates of the studies, error bars are 95% CIs and diamonds represent pooled summary estimates (whose width is their 95% CI).
Discussion
In our systematic review and meta-analysis of 10 neuropathological cross sectional or case control studies involving 481 cases and 3219 controls, we found a significant association between CAA and lobar ICH but not with ICH in other locations (figure 2).
This association between CAA and lobar ICH might have been even stronger had the included studies accounted for potential confounding factors (eg, age, severity of cognitive impairment, ethnic origin and possibly prior ischaemic stroke),40 included a consistent definition of ‘lobar’ ICH16 and focused on the prevalence of severe CAA (and other vasculopathic features, such as microaneurysms) in the blood vessels that were anatomically related to the ICH. The association might also have been stronger had the cases been selected according to the Boston diagnostic criteria, which ‘definitely’ attribute the cause of lobar ICH to CAA if there is pathological evidence of severe CAA with vasculopathy at postmortem.13 41 42 The Boston criteria for ‘probable CAA’ have an excellent specificity and therefore do not misclassify people who have lobar ICH without underlying severe CAA (100%, 95% CI 77% to 100%),13 but the sensitivity of these criteria for ‘probable CAA’ was 44% (95% CI 28% to 62%) and their negative predictive value was 39% (95% CI 22% to 58%), because more than half of the people with lobar ICH and severe CAA were not identified by the ‘probable’ criteria.13 Both systematic use of GRE MRI to identify brain microbleeds and the inclusion of superficial siderosis in the Boston criteria have improved their diagnostic accuracy42 but false positives and false negatives still exist and the role of other degrees of CAA severity in causing lobar ICH remains to be clarified, given that the studies in this meta-analysis were unable to do so.
This meta-analysis benefited from thorough ascertainment of pertinent studies, comprehensive critical appraisal to determine their inclusion, clarification by correspondence with study authors and a large number of cases and controls in our analyses. It is reassuring that our finding of an overall association between lobar ICH and CAA was confirmed by the three studies in which minimal confounding by patient age was evident.14 31 34 Unfortunately, only three of the included studies assessed the association of CAA and ICH having taken other competing risk factors for ICH into account,14 31 36 and just two studies described the influence on the association of other potential effect modifiers (Alzheimer-type pathology35 and antithrombotic drugs).14 Further confirmation of the direction of this association between CAA and lobar ICH, and exploration of the strength of the association, could only arise from further research with an ideal study design (box 1), given that an individual patient data meta-analysis was impossible.
The prevalence of CAA in patients with lobar ICH and the strength of the overall association between CAA and lobar ICH (figure 2), as well as the diagnostic accuracy of the Boston criteria for ICH due to CAA,13 42 are consistent with CAA being one of several potential causes of lobar ICH in the elderly. Although we have demonstrated an association between CAA and lobar ICH, this does not necessarily imply causation. Of Sir Austin Bradford Hill's nine criteria43 that would support an association being causal (see supplementary table 4, available online only), CAA is a plausible cause of lobar ICH,44 but further work is required to more reliably establish the association's strength, demonstrate its consistency and evaluate its biological gradient.43 If the methodological problems noted above are addressed and cases of lobar ICH are carefully phenotyped (according to their history of transient neurological events and cognitive impairment, and the presence of strictly lobar brain microbleeds on GRE MRI and superficial siderosis),42 then the strength of the association between CAA and lobar ICH would likely be much stronger. However, understanding whether milder degrees of CAA are associated with lobar ICH is also important to investigate the biological gradient and explore whether there are interactions with CAA of milder severity that might precipitate ICH.
Future research should include well designed case control and cohort studies to explore the CAA–ICH association (and its effect modifiers),37 individual patient data meta-analyses of comparable studies, further comparisons of the sensitivity and specificity of different methods of CAA detection (such as Congo Red staining versus immunohistochemistry)45 and the development and validation of a unified rating scale for CAA distribution and severity.46
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Neshika Samarasekera talks about hte paper in the JNNP podcast
Footnotes
Funding NS was funded by a clinical research training fellowship from the UK Medical Research Council and The Stroke Association. RASS was funded by a clinician scientist fellowship from the UK Medical Research Council.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.